Haeundae Paik Hospital, Inje University College of Medicine Busan, South Korea
Disclosure information not submitted.
Sunggun Lee1, Minkyoung Oh2, Mi-Yeong Kim3, Minyoung Her1 and Seong-Ho Kim1, 1Department of Internal Medicine, Haeundae Paik Hospital, Inje University College of Medicine, Busan, South Korea, 2Department of pharmacology, Inje University College of Medicine, Busan, South Korea, 3Department of Internal Medicine, Busan Paik Hospital, Inje University College of Medicine, Busan, South Korea
Background/Purpose: The association between symptomatic knee osteoarthritis (OA) and higher cardiovascular disease (CVD) mortality is well established; however, findings from previous studies that utilized regression analysis were limited, attributed to the strong association between OA and metabolic risk factors. This study aimed to evaluate the association between knee OA and mortality through propensity score matching.
Methods: This was a cohort study including Korean National Health and Nutrition Examination Survey (2010–2013) participants aged ≥50 years who had undergone screening knee radiographs (N=13087). By linking the survey data to Cause of Death data (through 2019) from Statistics Korea, mortality and cause-specific mortality data were obtained. Radiographic knee OA (ROA) was defined as bilateral Kellgren-Lawrence grade ≥2.Propensity score matching (1:1) was conducted between asymptomatic ROA, knee pain (without ROA), and symptomatic ROA groups and normal groups, balancing confounding factors (age, sex, obesity, hypertension, diabetes, total cholesterol, household income, history of stroke, history of MI). Time to death was analyzed using Cox Proportional hazard modeling. Sensitivity analysis was performed excluding those who died in a year of the observation period.
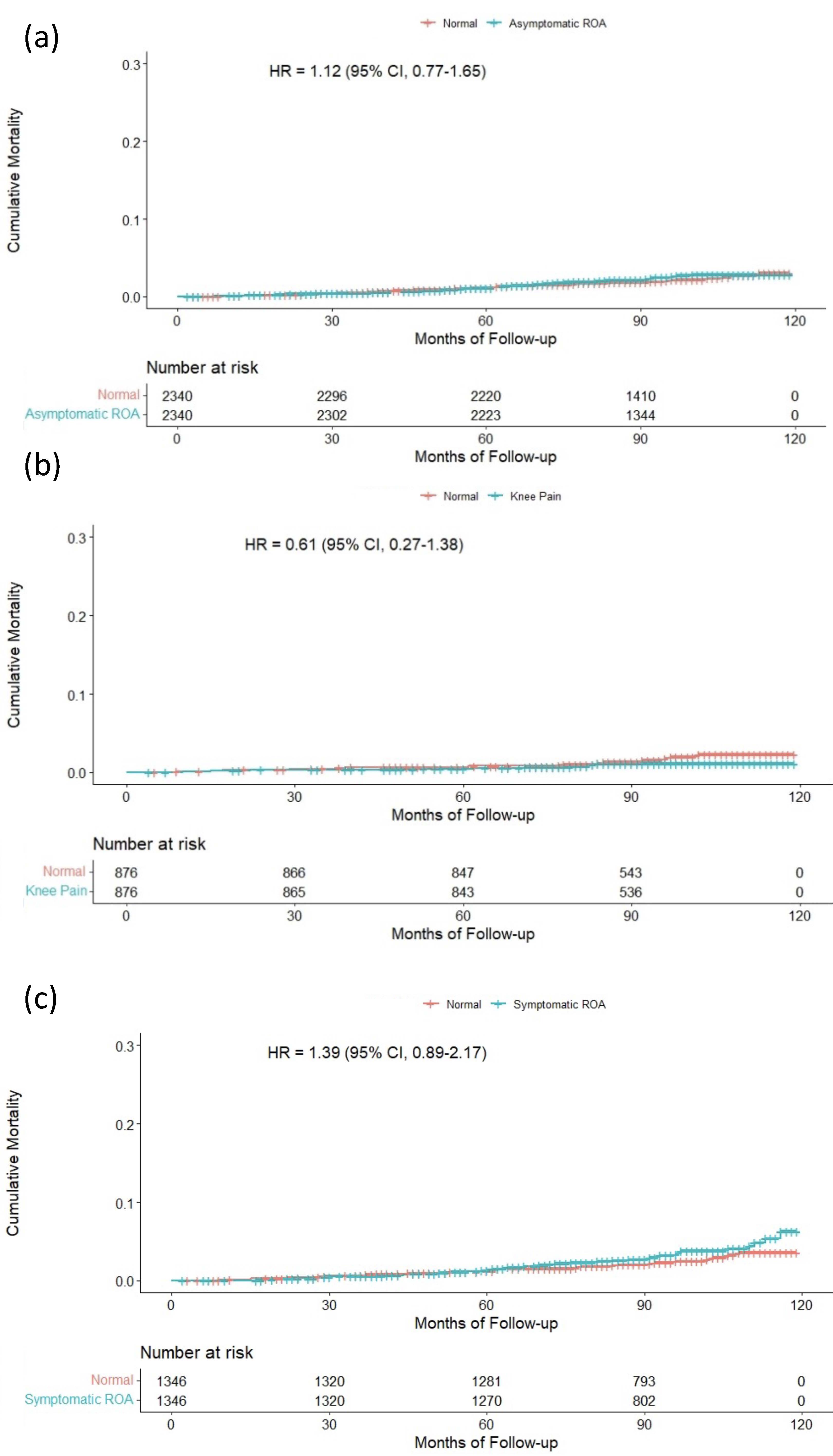
Results: The median and range of follow-up duration was 95 (0-124) months, and the total observation period was 103,330 person-years. There were 1128 deaths in the observation period. Crude mortality rates were higher in the ROA groups. All-cause mortality rate was 0.87, 1.32, 1.08, and 1.48 per 1000 patient-year in the reference, asymptomatic ROA, knee pain, and symptomatic ROA group, respectively. After matching there was a trend for higher CVD mortality in symptomatic ROA group, but not in other groups (Table 1 and Figure 1); the risk estimates were asymptomatic ROA HR 1.12 (95% CI 0.77–1.65), knee pain 0.61 (0.27–1.38), and symptomatic ROA 1.39 (0.89–2.17). There was no association between all-cause/cancer mortality and any group. In sensitivity analysis, there was a closer trend for higher CVD mortality in symptomatic ROA group (Table 1). The risk estimate was HR 1.48 (0.94–2.33).
Conclusion: When propensity score matching controls risk factor imbalances, the association between symptomatic knee OA and higher CVD-mortality was weaker compared with results of prior studies that used regression adjustment, and knee pain without radiographic OA was not associated with CVD mortality. Assuming that matching is a stronger method to control confounding variables and bias, the results may be more precise estimates of the total risk of knee OA for mortality, especially in East Asian population. Mediating effects by metabolic dysregulation merits further research.
Figure 1. Kaplan–Meier plot of cumulative mortality from cardiovascular disease up to 10 years for propensity score-matched participants with (a) asymptomatic ROA, (b) knee pain without ROA, and (c) symptomatic ROA. ROA, radiographic knee osteoarthritis.
S. Lee: None; M. Oh: None; M. Kim: None; M. Her: None; S. Kim: None.



.jpg)