Samsung Changwon Hospital Changwon-si, South Korea
Disclosure information not submitted.
Jiwon Hwang1, Sungjun Hong2, Kyunga Kim3, Jinhee Hur4, Yoosoo Chang5, Joong Kyong Ahn6 and Mira Kang7, 1Division of Rheumatology, Department of Internal Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon-si, South Korea, 2Department of Digital Health, Samsung Advanced Institute of Health Sciences and Technology (SAIHST), Sungkyunkwan University, Seoul, South Korea, 3Department of Digital Health, Samsung Advanced Institute of Health Sciences and Technology (SAIHST), Sungkyunkwan University; Biomedical Statistics Center, Data Science Research Institute, Research Institute for Future Medicine, Samsung Medical Center; Department of Data Convergence & Future Medicine, Sungkyunkwan University School of Medicine, Seoul, South Korea, 4Department of Food Science and Biotechnology, Sungkyunkwan University; Food Clinical Research Center, Institute of Biotechnology and Bioengineering, Sungkyunkwan University, Suwon, South Korea, 5Center for Cohort Studies, Total Healthcare Center, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine; Department of Occupational and Environmental Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, South Korea, 6Division of Rheumatology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, South Korea, 7Department of Digital Health, Samsung Advanced Institute of Health Sciences and Technology (SAIHST), Sungkyunkwan University; Health Promotion Center, Samsung Medical Center, Sungkyunkwan University School of Medicine; Digital Transformation Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea
Background/Purpose: Alcohol intake has been known to be interrelated with hyperuricemia and gout. However, the results of its influence are conflicting on serum uric acid (SUA) levels in terms of the beverage types and drinking amount. The study aimed to assess the impact of alcohol on SUA levels concerning the types of beverages and the drinking amount and habits in a large number of Korean populations.
Methods: We evaluated 17,011 adults who underwent comprehensive health examinations between 2011 and 2016. A standard drink unit for alcohol intake in Korea is defined as 8g based on the WHO definition. The dominant beverage was defined as the type of alcoholic beverage that was taken up more than 75% of total alcohol intake among beer, soju (Korean traditional liquor), and wine. Drinking habits were compared using the proportion within the same group of dominant liquor. Alcohol intake was categorized into six groups: none (0), almost none (0.01–0.49), little (0.50–0.99), light (1.00–1.99), moderate (2.00–3.99) and heavy (≥4.00) in the standard drink unit. The effect of alcohol consumption on SUA levels was investigated using linear regression models. Interaction effects were investigated in the subgroup analyses of sex and BMI.
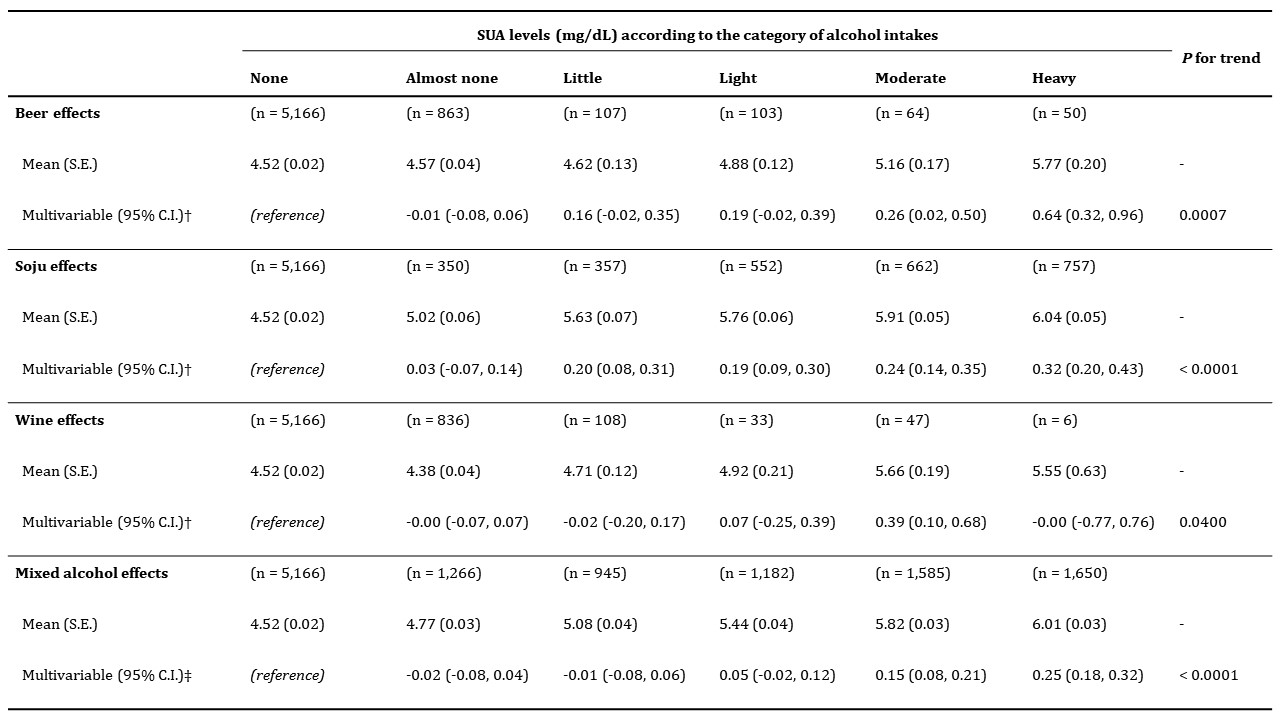
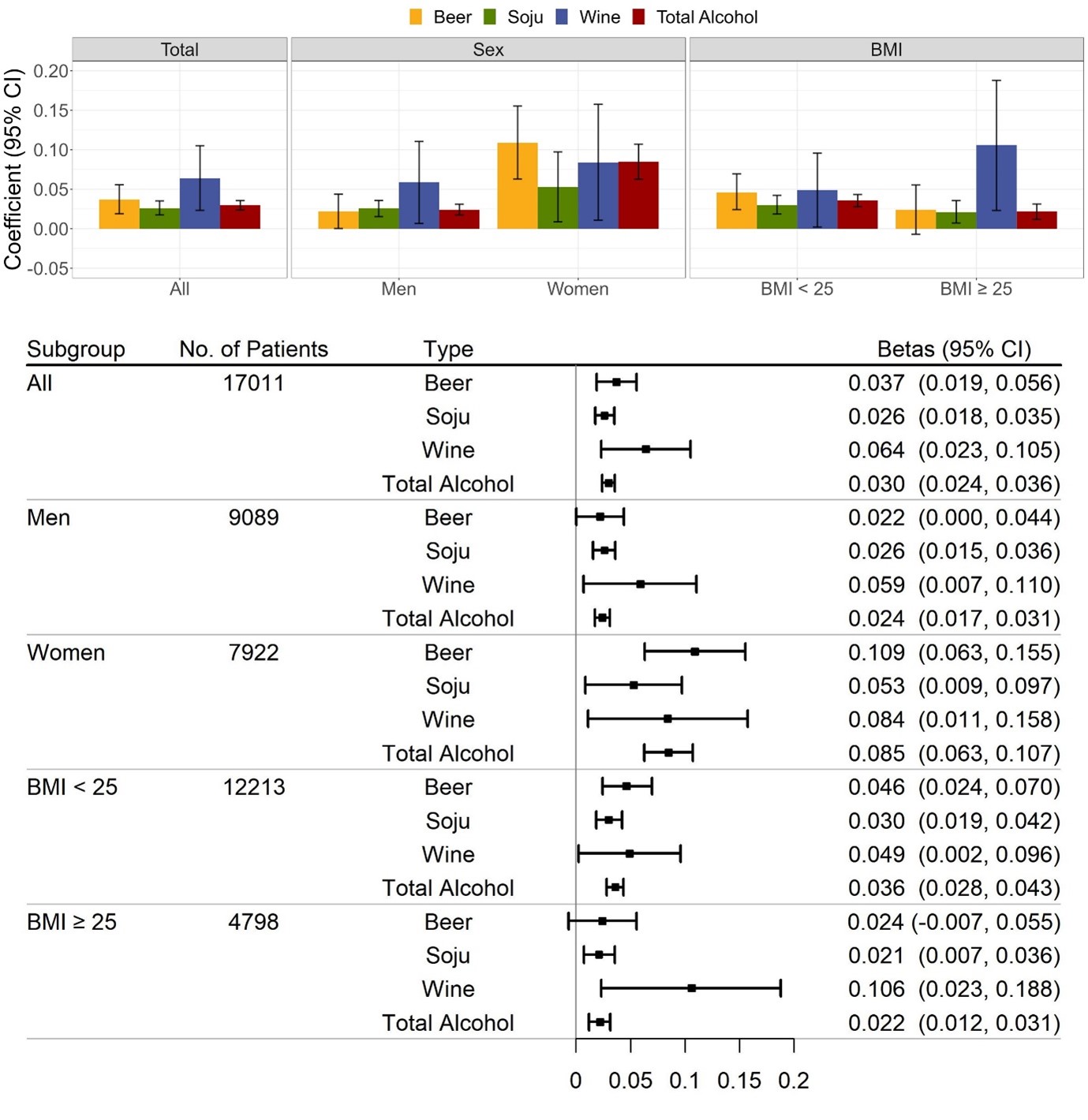
Results: The mean age of participants was 51.67±7.10 years, with 53.4% of men, and 69.6% of drinkers. The mean SUA level was 5.12±1.36 mg/dL and drinkers had significantly higher SUA, BMI, creatinine, low-density lipoprotein cholesterol, energy intake, and total protein intake (p< 0.05). Men's dominant beverage was soju, within which the proportion of heavy and mixed intake was noticeably higher. Women's dominant beverage was beer, within which the proportion of almost non-drinking was remarkable. SUA levels according to the six categories of alcohol intake were positively associated in a dose-dependent manner (p for trend< 0.001) irrespective of the beverage types and the association of beer and wine was weakened but still significant after adjusting in multivariable models. The total alcohol effect on SUA levels was greater in women compared to men: 0.26 [95% CI, 0.15-0.38] vs. 0.10 [0.01-0.18] mg/dL for the moderate drinking category and 0.53 [0.34-0.71] vs. 0.19 [0.11-0.27] mg/dL for the heavy drinking category (women vs. men). A significant change in SUA levels attributable to an association with alcohol intake was observed in beer, soju, and wine (0.039 [95% CI, 0.020-0.057], 0.028 [0.019-0.037], and 0.068 [0.027-0.108] mg/dL per standard drink unit per day). This effect on SUA levels differed in regard to the types of dominant beverages in men and women. Both sex and BMI had significant interactions with the alcohol effect on SUA levels. The modifying effects of alcohol intake were higher in women than those in men regardless of the beverage types. The interactions were also higher in subjects with BMI < 25 than in those with BMI ≥ 25, consistently across all types of beverages except wine.
Conclusion: Alcohol intake could have a significant dose-dependent association with SUA levels in both men and women, irrespective of the beverage types of alcohol and drinking habits. These findings may support healthcare providers to guide and educate subjects having hyperuricemia and gout in terms of alcohol intake.
Table 1. Associations between SUA levels and alcohol intakes of dominant groups in total. † Adjusted for other alcoholic beverages, age, sex, BMI, creatinine, LDL-C, hypertension, DM, alcohol-free calorie intake, and total protein intake ‡ Adjusted for age, sex, BMI, creatinine, LDL-C, hypertension, DM, alcohol-free calorie intake, and total protein intake
Figure 1. Associations between SUA levels and alcohol intakes in the sex and BMI subgroups. Interactions were significant for intake of beer, soju and total alcohol in the BMI subgroup, and for intake of beer and total alcohol in the sex subgroup (P values for interaction < 0.05). All other P values for interaction were greater than 0.05. Error bars represent 95% confidence intervals.
J. Hwang: None; S. Hong: None; K. Kim: None; J. Hur: None; Y. Chang: None; J. Ahn: None; M. Kang: None.