Session: (1734–1775) RA – Etiology and Pathogenesis Poster
1765: Persistent Cigarette Smoking Is Associated with Rheumatoid Arthritis Onset and Neutrophil Activation in a Prospective Study of At-risk First-Degree Relatives
Jeba Maisha, Xiaobo Meng, Hani El-Gabalawy and Liam O'Neil, University of Manitoba, Winnipeg, MB, Canada
Background/Purpose: Cigarette smoking (CS) is a major environmental risk factor for the development of Rheumatoid Arthritis (RA), and is associated with the development of RA autoantibodies, such as anti-citrullinated protein antibodies (ACPA) and rheumatoid factor (RF). However, it remains unclear what role(s) smoking has in the pathogenesis of RA, particularly during the pre-clinical stage. Using clinical, proteomic and in-vitro approaches, we sought to better understand the relationship between CS and RA onset in a large, prospective cohort of unaffected First-Degree Relatives (FDR) of RA patients, some of whom progressed to develop RA (Progressors).
Methods: Over the past 15 years, we established a longitudinal cohort of FDR of RA patients with a view to detect and predict incident RA. At baseline, and at each subsequent study visit, a CS questionnaire was administered, which included questions regarding past and current CS, and CS intensity. Based on these data, longitudinal CS patterns were extracted and related to demographics and autoantibody profiles. A previously published (32770634) discovery serum proteomic dataset (SOMAscan, 1288 proteins) was analyzed to explore the potential effect of smoking on the proteome of FDR. Neutrophils from healthy donors were stimulated with CS extract (CSE) and analyzed by flow cytometry, enzymatic profiling, immunofluorescence, protein citrullination and extracellular DNA release (SYTOX green).
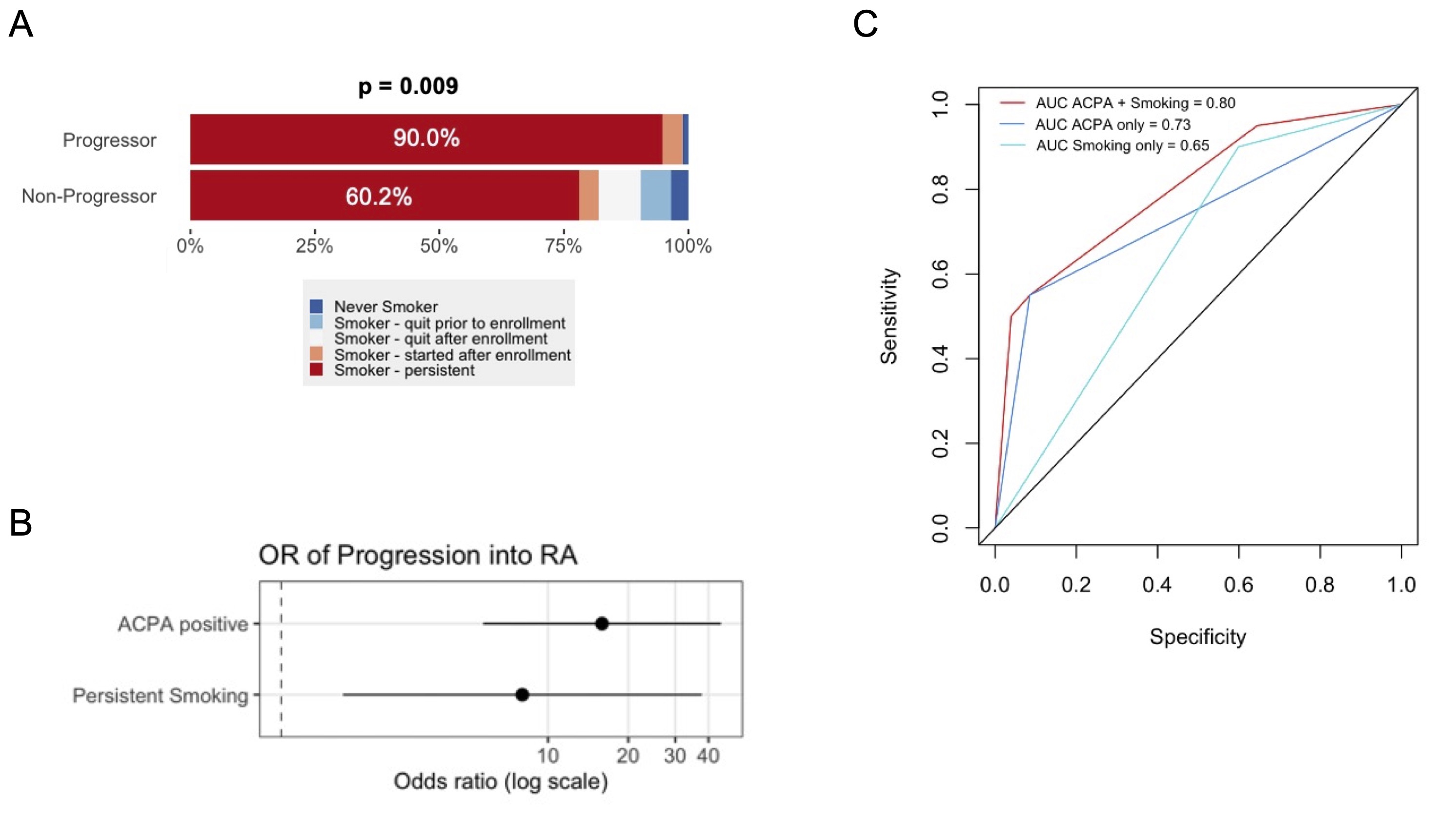
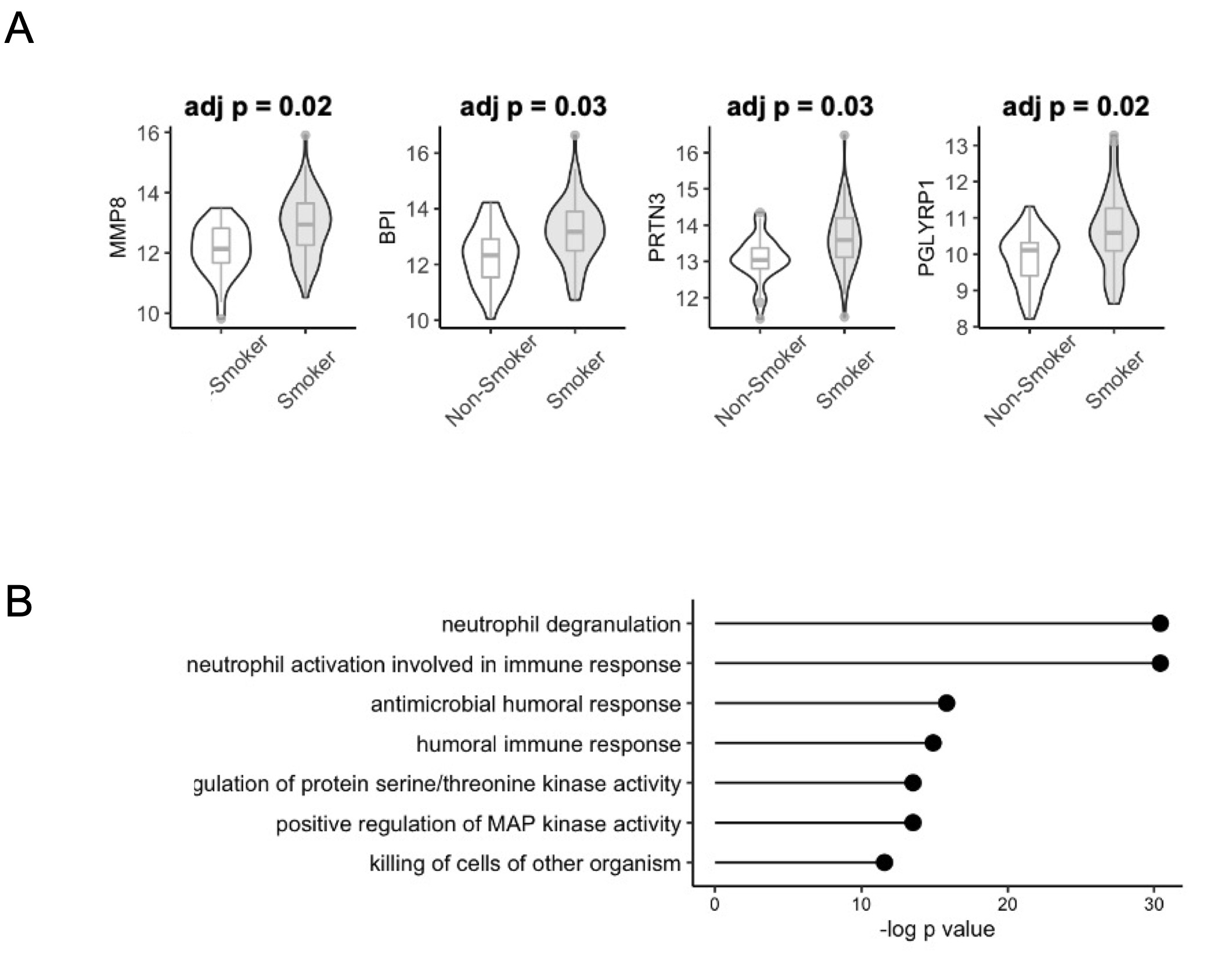
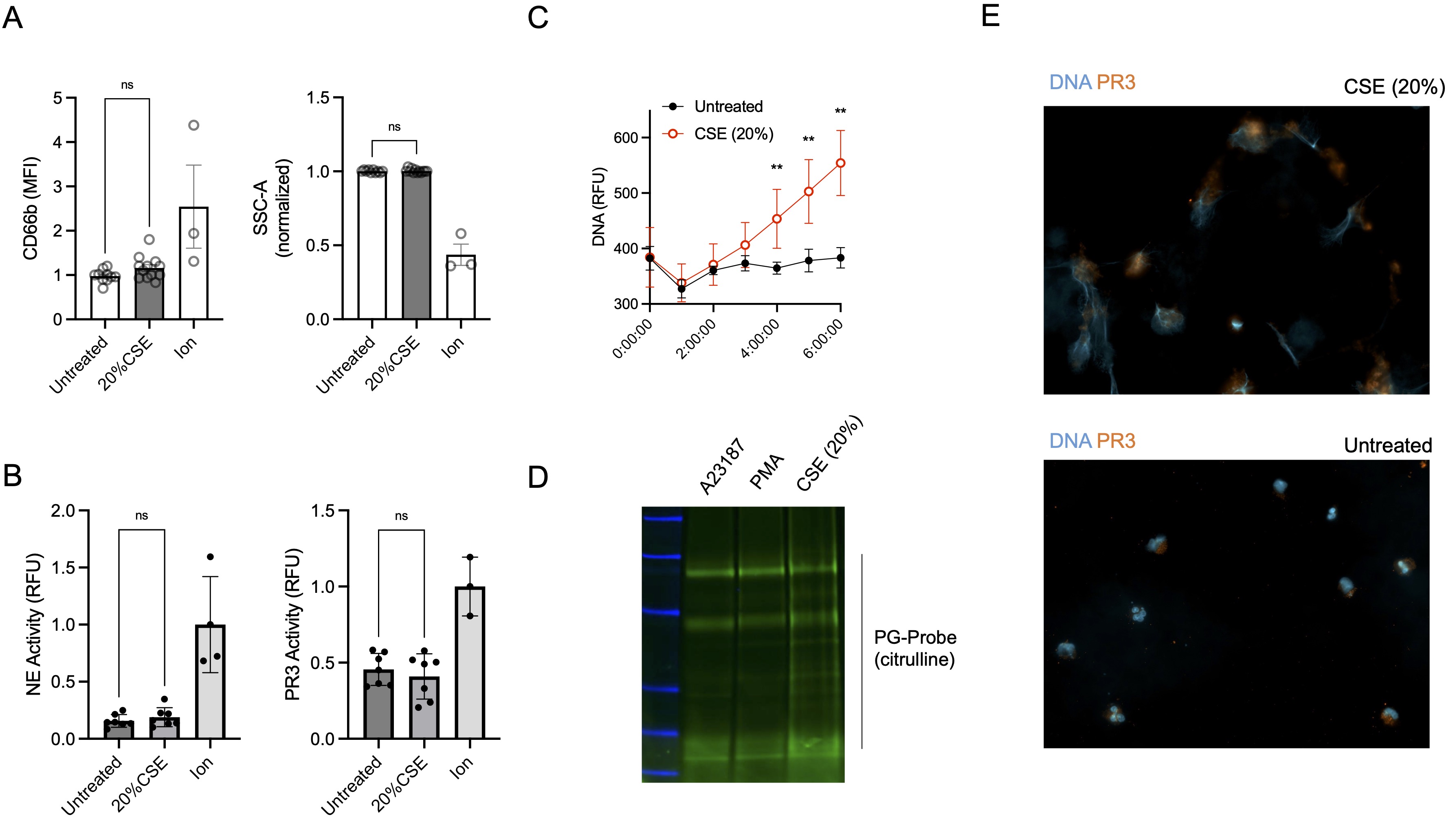
Results: In total, we were able to analyze CS patterns on 569 FDR, 19 of whom were Progressors. At baseline, current (79.6%) and ever (85.0%) CS rates were high in the study population, though neither was clearly associated with ACPA and/or RF seropositivity. Furthermore, baseline CS parameters did not predict future development of RA in the Progressors (n = 19). However, longitudinal CS patterns were strongly associated with Progression (Figure 1A, p = 0.009), with higher rates of persistent smoking in Progressors (90.0% vs 60.2%). In a logistic regression model, both persistent smoking (OR 8.0, 1.7 - 37.7) and ACPA positivity (15.9, 5.7 - 44.5) were independently associated with Progression (Figure 1B, C). Proteomic analysis and pathway enrichment suggested an upregulation of neutrophil proteins (Figure 2A) and neutrophil degranulation (p=5.2E-18, Figure 2B) in active smokers. Neutrophils cultured in-vitro with CSE (20%) skewed neutrophils away from degranulation (Figure 3A, B) and toward neutrophil extracellular trap (NET) formation, leading to the release of neutrophil proteases, extracellular DNA and citrullinated proteins (Figure 3C, D, E).
Conclusion: We show that persistent CS rather than incident CS was associated with RA development in a cohort of at-risk FDR of RA patients. Serum proteomics suggested that neutrophils are activated in smokers and neutrophils treated with CSE release NETs, but do not degranulate. These data suggest a potential mechanism by which smoking may stimulate neutrophils to undergo NET formation, and release citrullinated antigens and inflammatory proteins, which may in turn increase the risk of progression to clinically detectable RA.
Figure 1: Persistent cigarette smoking is associated with Rheumatoid Arthritis (RA) development in at-risk First-Degree Relatives (FDR). (A) Longitudinal rates of smoking persistence, cessation and abstinence in Progressor and Non-Progressor FDR. Analyzed as an ordinal variable with Wilcoxon Rank-Sum test. (B) Odds Ratio (OR) of anti-citrullinated protein antibody positivity (ACPA) and smoking persistence for Progression into RA. (C) Area under the curve (AUC) for Smoking (teal), ACPA (blue) and Both (red) for RA Progression.
Figure 2: Smoking in at-risk First-Degree Relatives (FDR) of Rheumatoid Arthritis (RA) patients is associated with neutrophil activation. (A) Serum protein expression (SOMAscan) of matrix metalloproteinase-8 (MMP8 aka. neutrophil collagenase), bactericidal/permeability-increasing protein (BPI), proteinase-3 (PRTN3), and peptidoglycan recognition protein 1 (PGLYRP1). (B) Gene ontology enrichment scores ordered by -log p-value for significant (p < 0.05) upregulated proteins in smokers (FC > 1) compared to non-smokers.
Figure 3: Neutrophils treated with cigarette smoke extract (CSE) skew towards neutrophil extracellular trap (NET) formation. (A) Neutrophils treated with CSE (20%) for 60 minutes do not upregulate CD66b (left, normalized) or display reduced side scatter (SSC, right), both surrogate markers of degranulation. Ion = A23187 (B) Protease activity for Proteinase-3 (PR3) and neutrophil elastase (NE) measured by enzyme kinetics by fluorescence in cell culture supernatant (60 minutes). Measured by Wilcox Rank-Sum Test (C) Cell-free DNA release over time measured by fluorescence (SYTOX green 0.2 µM), analyzed by multiple Mann-Whitney tests (** p < 0.01). (D) Protein citrullination in NETs (isolated after 4 hours in culture) measured by labeling with a Phenylglyoxal probe (PG) and in-gel fluorescent imaging. A23187 = Calcium Ionophore, PMA = phorbol myristate acetate (E) Immunofluorescence of images of CSE and untreated cells (4 hours) and stained for DNA (Hoescht, blue) and PR3 (orange).
J. Maisha: None; X. Meng: None; H. El-Gabalawy: None; L. O'Neil: None.