Session: (2387–2424) Vasculitis – Non-ANCA-Associated & Related Disorders Poster III
2415: Giant Cell Arteritis Is Associated with Worse Hospital Outcomes in Aortic Aneurysm/Dissection Hospitalizations: A Nationwide United States Population-Based Study
Loma Linda University Health San Bernardino, CA, United States
Disclosure information not submitted.
Artem Minalyan1, Christopher Hino1, Emily He1, Osahon Idolor2, Chinenye Osuorji3, Nneka Chukwu4, Ehizogie Edigin1 and Vaneet Sandhu5, 1Loma Linda University Health, Loma Linda, CA, 2Piedmont Athens Regional Hospital, Atlanta, GA, 3Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY, 4Nuvance Health Internal Medicine Residency, Poughkeepsie, NY, 5Loma Linda University, Loma Linda, CA
Background/Purpose: Giant Cell Arteritis (GCA) is a known risk factor for Aortic Aneurysm/Dissection (AAD). However, it is unclear if patients with GCA have worse hospital outcomes when hospitalized for AAD compared to patients without GCA hospitalized for AAD. We queried the largest inpatient hospitalization database in the United States (U.S.) to answer this question.
Methods: Data were abstracted from the National Inpatient Sample (NIS) from 2016 to 2020 Database. NIS is a nationally representative approximate 20-percent stratified sample of all discharges from U.S. community hospitals, excluding rehabilitation and long-term acute care hospitals. The numbers in the databases are weighted to optimize national estimates. The NIS was searched for hospitalizations for patients aged ≥ 50 years with a principal diagnosis of AAD ("I71") with and without a coexisting secondary diagnosis of GCA ("M315" and "M316") using ICD-10 codes. The principal diagnosis is the main reason for hospitalization. Any diagnosis other than the principal is a secondary diagnosis. Each hospitalization in the NIS has only 1 principal diagnosis and can have up to 40 secondary diagnoses. The chi-square test was used to compare baseline characteristics between the GCA and non-GCA groups. The primary outcome was inpatient mortality. Hospital length of stay (LOS) and total hospital charges were secondary outcomes. Multivariable logistic and linear regression analyses were used to adjust for confounders for the primary and secondary outcomes, respectively. We adjusted for age, gender, race, insurance type, income, Charlson co-morbidity index, and hospital characteristics. STATA version 16 was used for analysis. Since NIS contains publicly available depersonalized data, Institutional Review Board (IRB) review was waived.
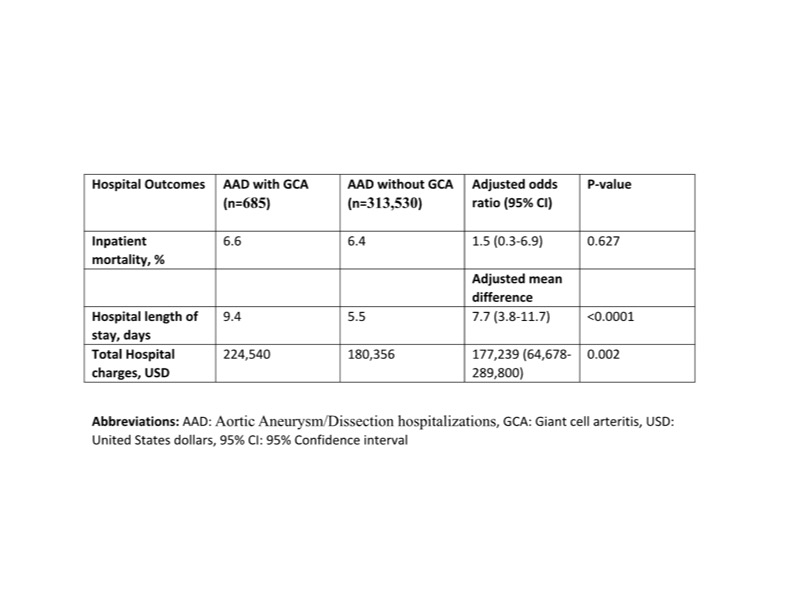
Results: There were about 175 million hospitalizations in the combined 2016-2020 database. We obtained 314,215 hospitalizations for patients aged ≥ 50 years with a principal diagnosis of AAD. 685 (0.2%) of these had a secondary diagnosis of GCA, while 313,530 (99.8%) did not have co-existing GCA. The GCA group was older (mean age of 74.6 vs 71.8 years, p < 0.0001) and had more females (76.6% vs 29.5%, p < 0.001) compared to the non-GCA group. The GCA group had similar inpatient mortality compared to the non-GCA group (6.4% vs 6.6%, p=0.627). The GCA group had longer LOS (9.4 vs 5.5 days, p < 0.0001) and higher total hospital charges ($224,540 vs 180,356, p=0.002) compared to the non-GCA group. See table 1.
Conclusion: GCA patients admitted for AAD have worse hospital outcomes (longer LOS and higher total hospital charges) compared to non-GCA patients admitted for AAD. Adequate treatment of GCA to prevent complications such as AAD is needed. In addition, screening, early detection, and prompt management of AAD via a multidisciplinary approach are essential in optimizing the outcomes of GCA patients.
Table 1: Hospital outcomes of Aortic Aneurysm/Dissection hospitalizations with and without Giant Cell Arteritis
A. Minalyan: None; C. Hino: None; E. He: None; O. Idolor: None; C. Osuorji: None; N. Chukwu: None; E. Edigin: None; V. Sandhu: Exagen, 2, 5.