Anne Bull Haaversen1, Tanaz Kermani2, Lene Kristin Brekke3, Oyvind Molberg4 and Andreas Diamantopoulos5, 1Martina Hansens Hospital, Hosle, Norway, 2Rheumatology, David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA, 3Haugesund Hospoital For Rheumatic Diseases, Haugesund, Nepal, 4Dept of Rheumatology, University Hospital Oslo, Oslo, Norway, 5Akershus University Hospital, Lørenskog, Norway
Background/Purpose: Patients with Giant cell arteritis (GCA) face an elevated risk of aneurysm formation. Despite this, consensus regarding optimal aortic visualization methods and aneurysm monitoring frequency is still lacking. Low-frequency transducer ultrasound offers a potential solution, capable of visualizing the ascending aorta and aortic arch. We conducted a study to compare this ultrasound technique against Computed Tomography Angiography (CTA), the current gold standard for aortic evaluation.
Methods: We conducted our study at Martina Hansens Hospital in Bærum, Norway. We included patients diagnosed with GCA who also met the ACR/EULAR classification criteria for GCA. The ascending aorta's diameter was measured using both ultrasound and CTA. Aortic aneurysm was defined as an ascending aorta diameter of ≥40 mm. The Student's t-test was used to compare the results.
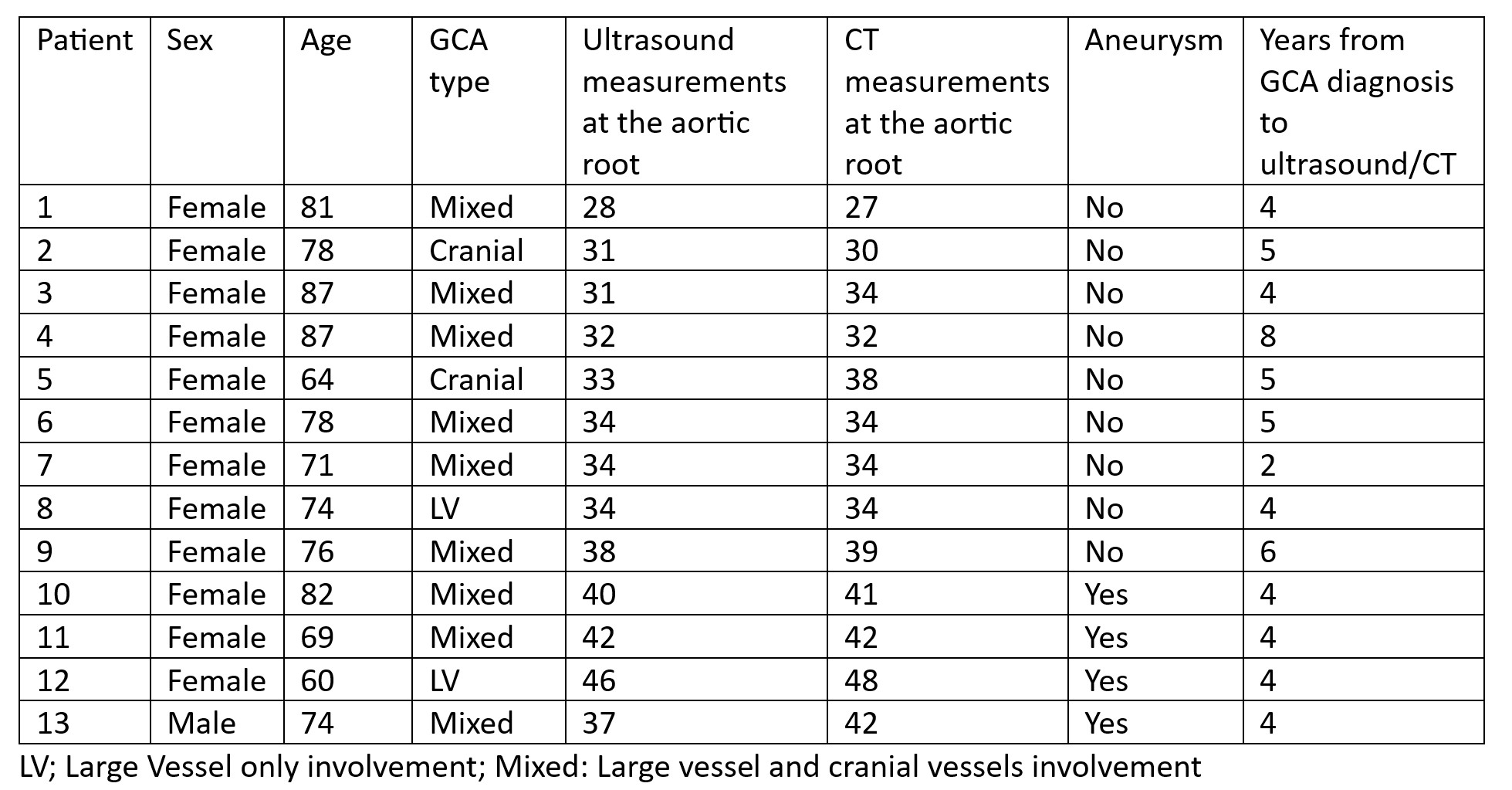
Results: Our pilot study included thirteen patients, twelve females, and one male, with an average disease duration of 4.6 years (95%CI 3.7-5.5). The mean diameter of the ascending aorta was 35.4 mm (95%CI 32.3-38.4) measured by ultrasound and 36.5 mm (95%CI 33.0-40.0) by CTA. The mean difference between the two methods was 1.15 mm (95%CI -0.07 to 2.38, p-value = 0.06). CTA identified four patients with an ascending aorta aneurysm, while ultrasound identified three. (Table 1). No aneurysms were found in the descending aorta by CTA.
Conclusion: Our preliminary findings suggest that ultrasound provides results comparable to CTA in assessing the ascending aorta diameter in GCA patients. This positions ultrasound as a potential tool for monitoring aortic aneurysm development in this patient group.
A. Bull Haaversen: None; T. Kermani: None; L. Brekke: None; O. Molberg: None; A. Diamantopoulos: None.