Northwestern University Chicago, IL, United States
Disclosure information not submitted.
Laura Arneson1, Biana Modilevsky2 and Anisha Dua1, 1Northwestern University, Chicago, IL, 2University of Arizona - Tucson / Banner University Medical Center, Tucson, AZ
Background/Purpose: Enhancing rheumatology education in Internal Medicine (IM) residency may encourage residents to pursue rheumatology careers, and promote familiarity with rheumatology among those entering other fields. A needs assessment of rheumatology training in IM residency was conducted at an academic program (A) and community program (B) in the same city in 2021. At baseline, all third-year residents at B rotated in a rheumatology clinic for one month; A had no required rheumatology rotation. Neither program had structured rheumatology didactics. Surveys of residents and analysis of In-Training Exam (ITE) scores guided development of a rheumatology curriculum. An assessment of curriculum outcomes after the first year is presented.
Methods: A baseline survey was sent to all IM residents at A and B in Spring 2021, with questions on amount of rheumatology training in residency, interest in learning about rheumatology, interest and confidence in specific topics, and preferred curriculum formats. Results informed the curriculum, implemented starting August 2021. Noon conferences about rheumatology labs and systemic lupus erythematosus (SLE) were delivered at A and B, including pre- and post-quizzes and reference handouts. At A, conferences were also delivered on spondyloarthropathies and vasculitis, and each intern was scheduled for one half-day in rheumatology clinic. The survey was repeated in Spring 2022. ITE scores before and after curriculum implementation were compared (Fall 2020 and 2022).
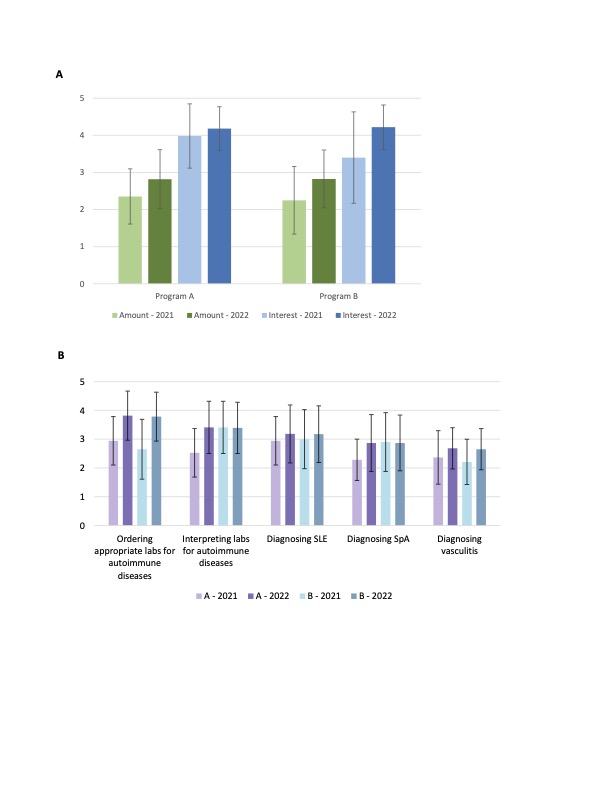
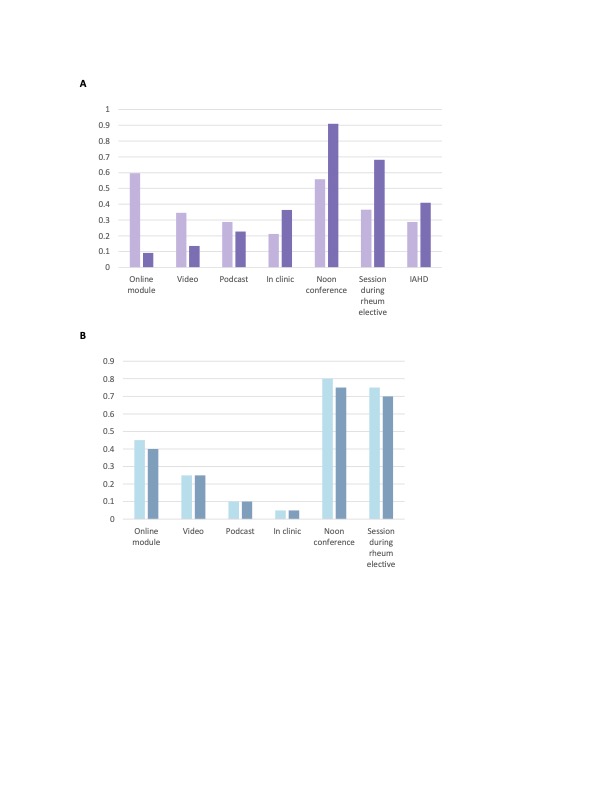
Results: Baseline surveys were completed by 46% of residents (n=53) at A and 87% (n=20) at B. Post-surveys were by completed by 19% of residents (n=22) at A and 100% (n=23) at B. From 2021 to 2022, ratings of amount of rheumatology training in residency, interest in learning about rheumatology, and confidence in topics covered in conferences increased non-significantly (Figure 1). Preference for in-person curriculum formats increased at A and remained high at B (Figure 2). During the conference on labs, average quiz score increased at A: 40% (n=17, SD 26%) to 74% (n=20, SD 20%), and at B: 27% (n=6, SD 10%) to 77% (n=5, SD 15%). For the conference on SLE, average quiz score increased at A: 42% (n=8, SD 15%) to 90% (n=6, SD 17%), and at B: 52% (n=11, SD 10%) to 93% (n=14, SD 13%). From 2020 to 2022, scores on the rheumatology portion of the ITE increased from 65th to 89th national percentile at A, and decreased from 5th to 4thpercentile at B. Ranking ITE performance in the 11 IM subspecialties by percentile, A's rheumatology scoreincreased from 10th to 3rd (tied) subspecialty, while B's decreased from 6th (tied) to 10th (tied).
Conclusion: Implementation of a rheumatology curriculum resulted in several advances after one year; outcomes varied between two programs. Residents demonstrated knowledge gains during conference sessions at both A and B. Rheumatology ITE score percentile improved only at A, which received additional didactics. Resident-reported metrics of their rheumatology training improved slightly at both. Preferred curriculum formats shifted from virtual to in-person from 2021 to 2022. Incomplete resident participation at A was a limitation. Next steps include adding additional conferences and reference materials.
Figure 1. Resident survey responses from internal medicine programs A and B, before and after implementation of a rheumatology curriculum. Pre-surveys (lighter bars) were conducted in Spring 2021 at A (n=53, response rate 46%) and B (n=20, response rate 87%). Post-surveys (darker bars) were conducted in Spring 2022 at A (n=22, response rate 19%) and B (n=23, response rate 100%). Error bars represent standard deviations. Panel A: Rating of the amount of rheumatology training received in residency on a 5-point Likert scale (1 = very inadequate, 5 = more than adequate) is shown in green; rating of interest in learning about rheumatology on a 5-point Likert scale (1 = not at all interested, 5 = very interested) is shown in blue. Panel B: Rating of confidence in rheumatology topics on a 5-point Likert scale (1 = not at all confident, 5 = very confident) is shown in purple for A and blue for B. SLE = systemic lupus erythematosus; SpA = spondyloarthropathies.
Figure 2. Resident preferences for format of a rheumatology curriculum in 2021 compared to 2022, at program A (panel A) and program B (panel B). Pre-surveys (lighter bars) were conducted in Spring 2021 at A (n=53, response rate 46%) and B (n=20, response rate 87%). Post-surveys (darker bars) were conducted in Spring 2022 at A (n=22, response rate 19%) and B (n=23, response rate 100%). Residents were asked to select 1-3 preferred formats; percent of residents selecting each format is shown. Rheum = rheumatology; IAHD = intern academic half-day, a format available only at A.
L. Arneson: None; B. Modilevsky: None; A. Dua: AbbVie/Abbott, 2, Amgen, 2, GlaxoSmithKlein(GSK), 2, Novartis, 2, sanofi, 2.