Monica Yang1, Seoyeon Lee2, Lisa Hazelwood3, Dean Sheppard1, Francesco Boin4 and Paul Wolters1, 1University of California San Francisco, San Francisco, CA, 2Yale University School of Medicine, New Haven, CT, 3AbbVie, Inc., North Chicago, IL, 4Cedars-Sinai Medical Center, Los Angeles, CA
Background/Purpose: Despite recent advances in systemic sclerosis (SSc), there remains a paucity of clinically actionable biomarkers to assess disease severity and predict progression. Collagen triple helix repeat containing-1 (CTHRC1), a protein secreted during tissue-repair that regulates fibroblast function and vascular remodeling after arterial injury has been reported to be a marker for a subpopulation of fibroblasts uniquely found in lungs of SSc-ILD patients. The aim of this study was to determine whether serum levels of CTHRC1 are associated with specific disease manifestations and predict clinical outcomes in SSc.
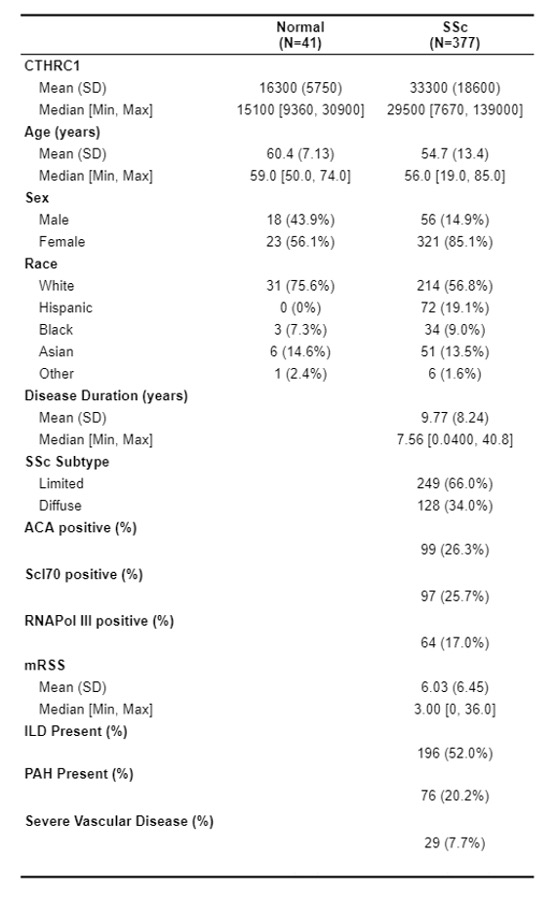
Methods: Retrospective analysis of a prospectively collected longitudinal cohort was performed using a large, well characterized cohort of SSc patients, fulfilling the ACR/EULAR 2013 classification criteria, and healthy controls. Serum levels of CTHRC1 were measured by ELISA in 377 SSc patients and 40 healthy controls (Table 1). SSc patients were stratified by quartiles of CTHRC1 serum level for analysis. Quartile characteristics were compared using ANOVA/Chi-Square and mixed models were utilized to assess the association of CTHRC1 serum level with SSc disease manifestations and severity, including skin disease, interstitial lung disease (ILD), pulmonary arterial hypertension (PAH), and peripheral vascular disease. Survival analysis, as defined by time to death or lung transplantation, was assessed by Kaplan-Meier analysis between quartiles with long-rank test.
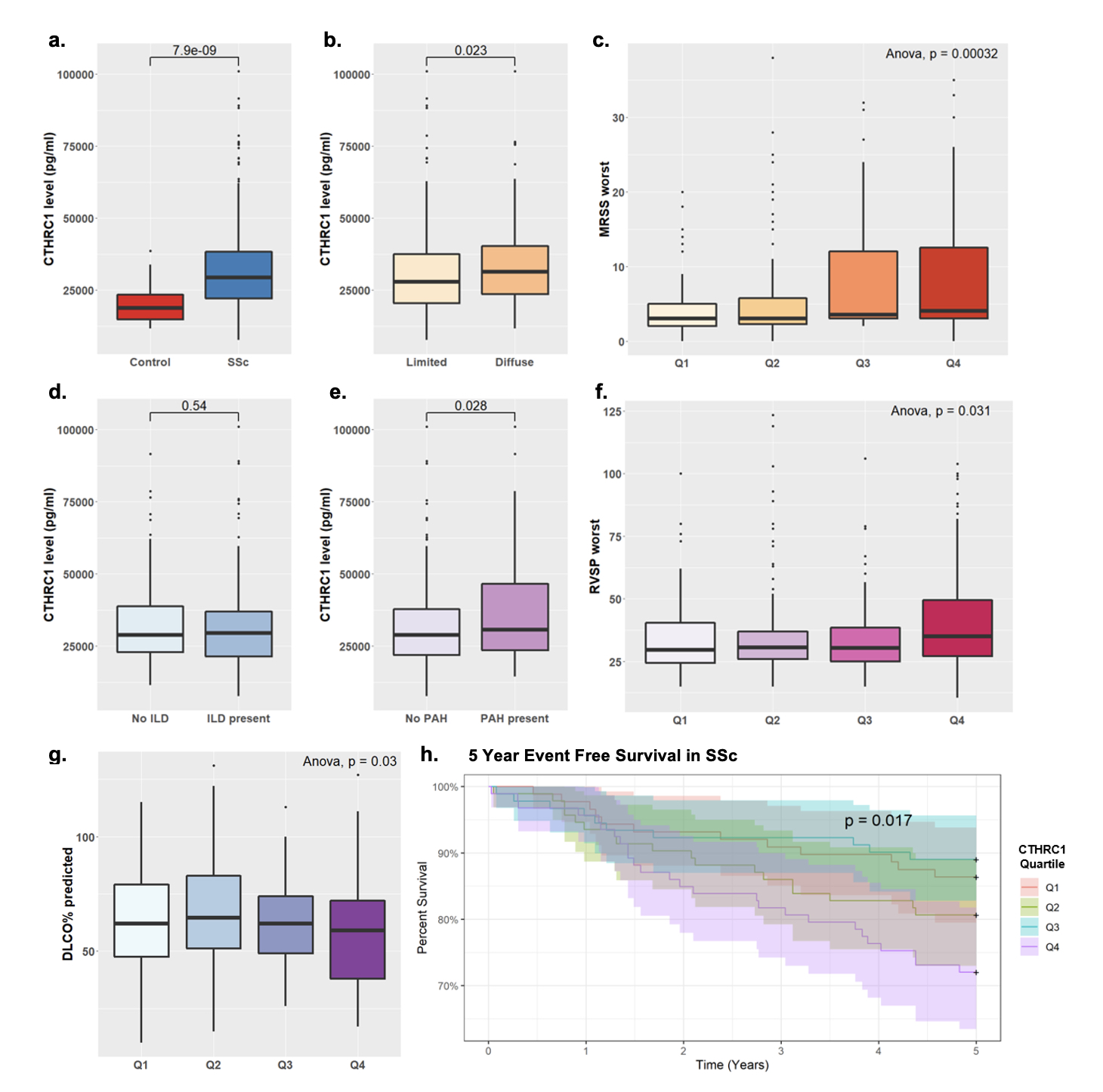
Results: Serum CTHRC1 was significantly increased in SSc patients compared to healthy controls (Fig 1a). After controlling for age, sex, race, disease duration and SSc antibody status, elevated CTHRC1 was independently associated with skin disease severity (p< 0.05) and PAH (OR=1.43 per 10k pg elevation, p=0.005). Patient with diffuse skin disease had significantly higher CTHRC1 than limited skin disease (p=0.023) (Fig 1b) and elevated CTHRC1 was associated with both increased MRSS at time of serum measurement (p=0.003) and worst MRSS recorded (p=0.005) (Fig 1c). CTHRC1 was not associated with the presence of ILD, however was significantly elevated in subjects with PAH (Fig 1d-e). After controlling for covariates, higher CTHRC1 levels were significantly associated with markers of PAH severity, including decreased DLCO% predicted (p< 0.001) and elevated RVSP (p=0.003) at time of serum measurement as well as for worst recorded values (p=0.01) (Fig 1f-g). Elevated CTHRC1 serum level was associated with worse survival among SSc patients (Fig 1h).
Conclusion: Circulating CTHRC1 levels are increased in SSc patients and exhibit a significant association with more severe skin disease, PAH, and worse survival. While it remains to be determined whether CTHRC1 is directly implicated in the disease pathologic process, these findings suggest that circulating CTHRC1 may be further validated as a clinically actionable biomarker in SSc.
Table 1: Demographic and clinical characteristics of SSc patients and healthy controls
Figure 1: Serum CTHRC1 levels are elevated in SSc patients (a) and associated with skin disease severity (b-c), PAH severity (d-g) and 5 year event free survival (h). Q1 represents quartile of patients with lowest serum CTHRC1 level while Q4 represents highest.
M. Yang: None; S. Lee: None; L. Hazelwood: AbbVie/Abbott, 3, 11; D. Sheppard: None; F. Boin: None; P. Wolters: None.