University of Pennsylvania Philadelphia, PA, United States
Disclosure information not submitted.
Kimberly DeQuattro1, Laura Trupin2, Sarah Patterson3, Stephanie Rush2, Caroline Gordon4, Kurt Greenlund5, Kamil Barbour5, Cristina Lanata6, Lindsey Criswell7, Maria Dall'Era2, Jinoos Yazdany2 and Patti Katz8, 1University of Pennsylvania, Media, PA, 2University of California San Francisco, San Francisco, CA, 3University of California San Francisco, Pacifica, CA, 4Institute of Inflammation and Ageing, University of Birmingham, Birmingham, United Kingdom, 5Centers for Disease Control and Prevention, Atlanta, GA, 6National Human Genome Research Institute, Washington, DC, 7NIH/NHGRI, Bethesda, MD, 8University of California San Francisco, San Rafael, CA
Background/Purpose: Trauma exposures are associated with SLE onset and disease activity; perceived stress is also associated with greater SLE disease activity and worse patient-reported outcomes. However, perceptions of stress vary in response to life events and may be influenced positively and negatively by psychosocial factors. In an SLE cohort, we examined the association of stressful events with perceived stress, whether psychosocial factors affected perceived stress, and whether these relationships varied by prior trauma exposures.
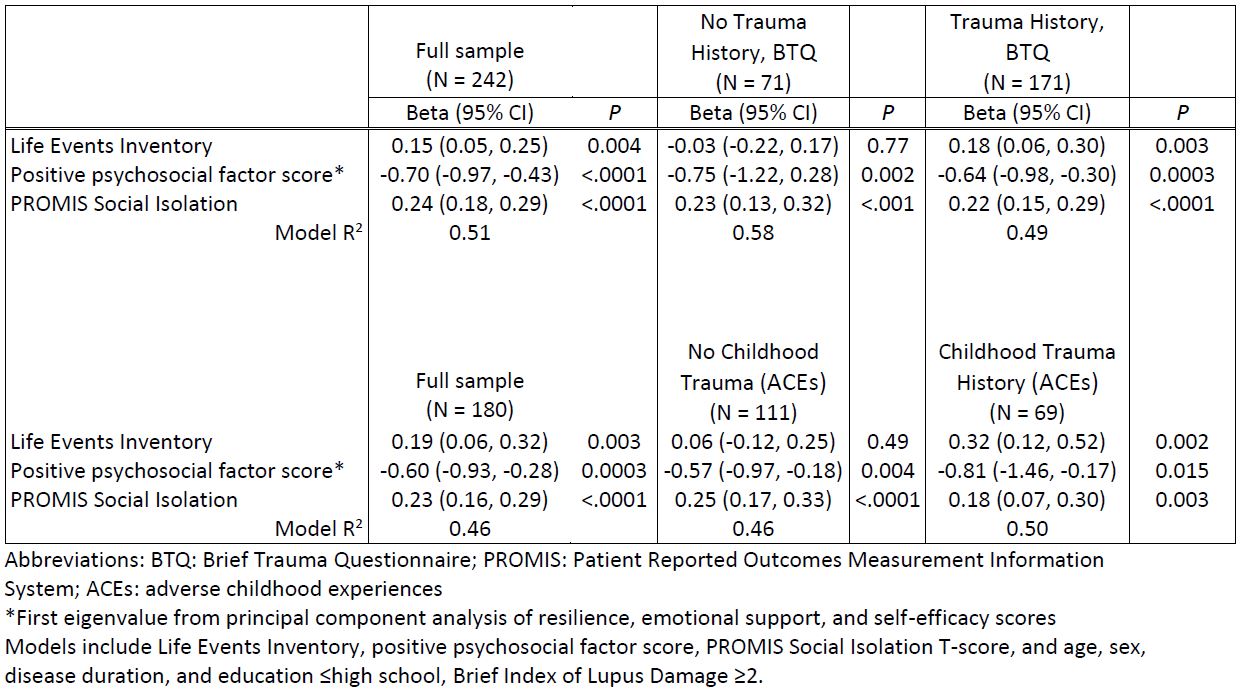
Methods: Data were from a sample of adults with SLE from the California Lupus Epidemiology Study (n = 242). We first examined correlations of stressful events that occurred in the past year (Life Events Inventory: queries potentially stressful health, living situation, family, financial, and legal events) and psychosocial factors (3 positive: resilience, self-efficacy, emotional support; 1 negative: social isolation) with perceived stress (Perceived Stress Scale). Because of high correlations among positive psychosocial variables, we used principal components analyses to create a positive psychosocial factor score. We then used multivariable linear regression to examine independent associations of stressful events and psychosocial variables with perceived stress, controlling for age, sex, disease duration, and educational attainment for the total sample and stratified by lifetime trauma history (Brief Trauma Questionnaire, BTQ; any traumatic event vs none). Analyses stratified by history of adverse childhood experiences (ACEs; 0-1 events vs ≥2 events) among the subset for whom ACEs data were available (n = 180) were performed.
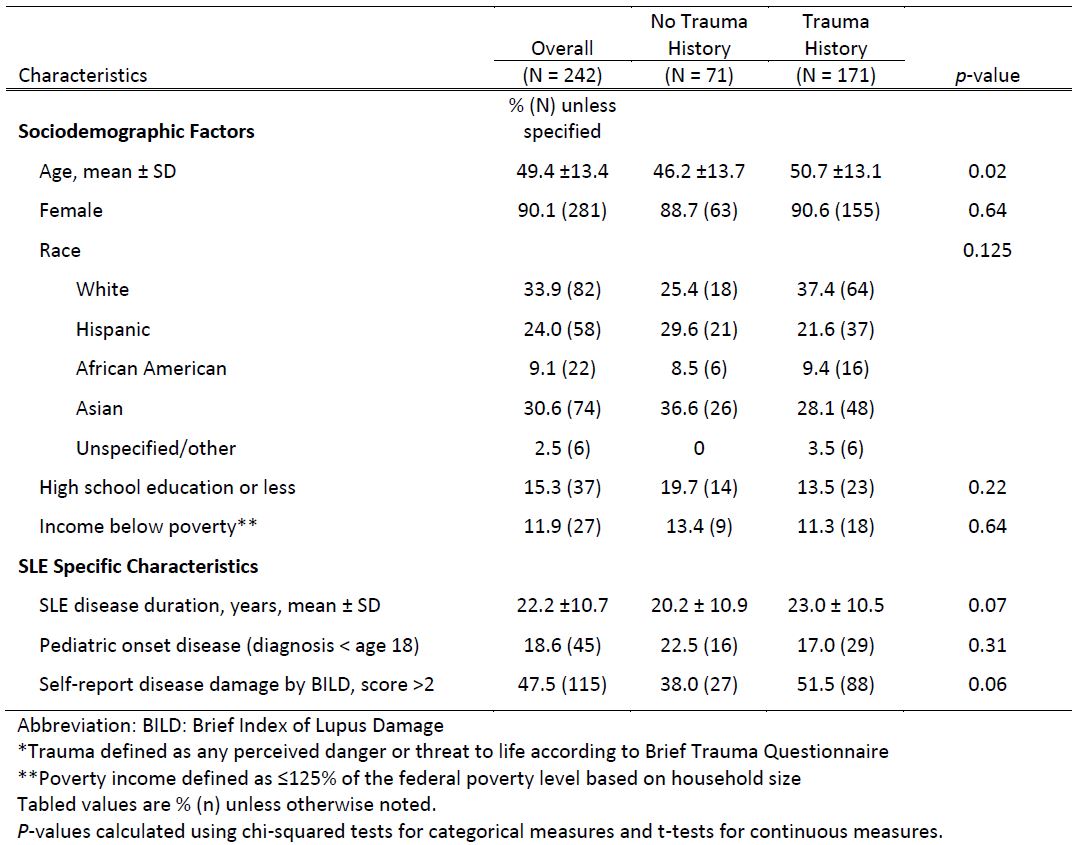
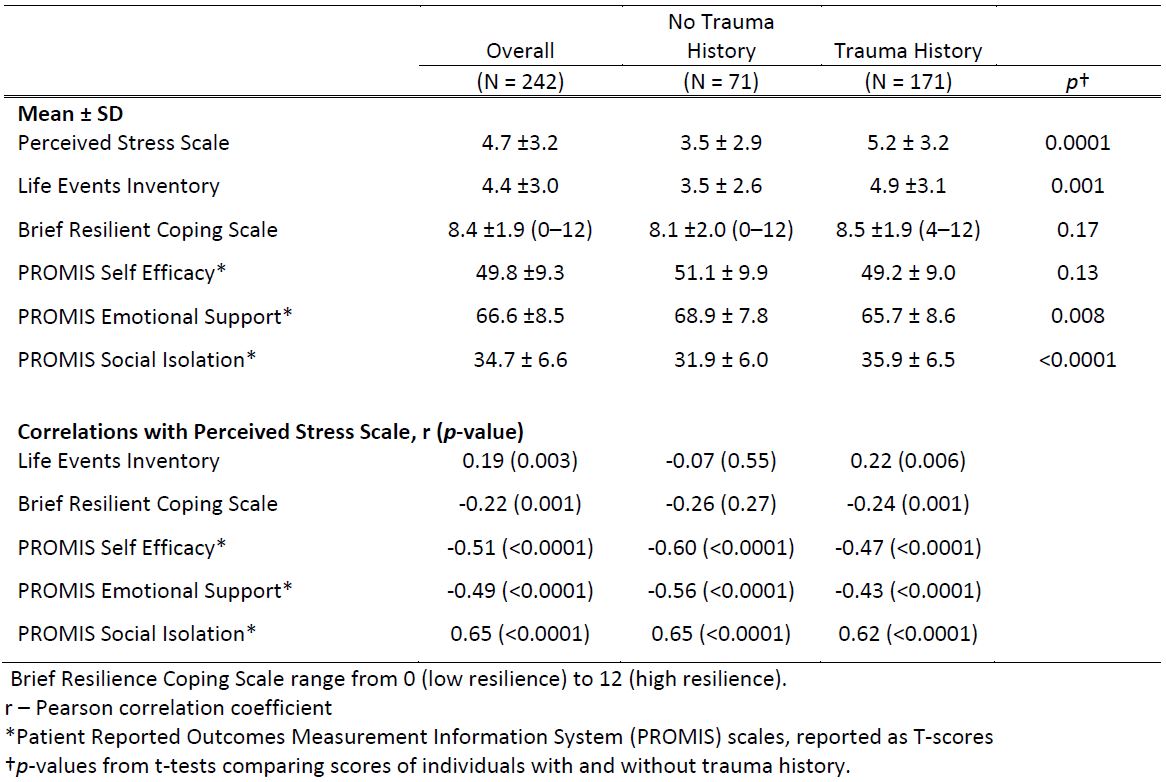
Results: Sample characteristics are shown in Table 1. Individuals who had experienced trauma (71%, BTQ) had significantly higher perceived stress scores, more stressful events, lower emotional support scores, and higher social isolation scores (Table 2). Overall, a greater number of stressful events over the previous year and social isolation were correlated with greater perceived stress, and positive psychosocial factors (resilience, self-efficacy, and emotional support) were associated with lower perceived stress (Table 2). In analyses stratified by BTQ trauma and ACEs (38%), associations of positive and negative psychosocial factors with perceived stress were similar between groups. However, the number of recent stressful life events was significantly associated with perceived stress only for people with BTQ trauma or ACEs (Table 3).
Conclusion: Perceived stress was higher in individuals with SLE with BTQ trauma and/or ACEs. Individuals with trauma history may be more vulnerable to current interpersonal, economic, or other stressful experiences that lead to higher perceived stress levels. Given demonstrated associations between perceived stress and poor health outcomes in SLE, modifiable positive psychosocial resources such as self-efficacy and emotional support may be important in managing perceptions of stress. Increased access to interventions that strengthen positive psychosocial factors and lessen negative ones to lower perceived stress is a next step towards improving outcomes in SLE.
Table 1. Characteristics of study participants with SLE, by trauma history*
Table 2. Association of Perceived Stress Scale with Life Events Inventory, measures of positive (resilience, self-efficacy, emotional support) and negative (social isolation) factors, by trauma history
Table 3. Association of perceived stress and stressful events (Life Events Inventory), measures of positive psychosocial and negative (social isolation) factors, by trauma history (Brief Trauma Questionnaire and adverse childhood experiences), in models with adjustment
K. DeQuattro: None; L. Trupin: None; S. Patterson: None; S. Rush: None; C. Gordon: AbbVie, 2, Alumis, 2, Amgen, 2, AstraZeneca, 2, Sanofi, 2, UCB Pharma, 2; K. Greenlund: None; K. Barbour: None; C. Lanata: None; L. Criswell: None; M. Dall'Era: Annexon Biosciences, 2, 5, AstraZeneca, 2, Aurinia, 2, Biogen, 2, GlaxoSmithKlein, 2, 5, Pfizer, 2; J. Yazdany: Astra Zeneca, 2, 5, Aurinia, 5, Gilead, 5, Pfizer, 2; P. Katz: None.