David Alfego1, Quinn Hlatky2, Stanley Naides3, Karis Lee4, Jennifer Ennis5 and Kristen Clark6, 1LabCorp, San Diego, CA, 2LabCorp, Philadelphia, PA, 3Labcorp, Dana Point, CA, 4LabCorp, Orlando, FL, 5LabCorp, Chicago, IL, 6LabCorp, Raleigh, NC
Background/Purpose: Rheumatologic disorders can take years to diagnose. Diagnosis often requires a combination of specific symptoms, examination findings and laboratory testing, rather than a single test. Additionally, symptoms presenting in rheumatologic processes are often present in other common conditions, making diagnosis challenging. A common starting point is an antinuclear antibody (ANA) test, often ordered by a non-rheumatology provider, followed by a wide range of further antibody testing to narrow disorders. Here, we sought to examine patterns of post-ANA testing using real world evidence to inform order guidance opportunities and help advance diagnosis.
Methods: De-identified data from the Labcorp® testing databasewere queried for all ANA orders (both individual and panel testing) between 2011 and 2022. Any ANA order placed by a rheumatologist was excluded. Follow-up antibody testing (such as Anti-Smith, Anti-dsDNA antibodies, etc.) within 365 days post-positive ANA result (1:80 or higher) and respective positivity rates were examined. Reason for ANA ordering was evaluated via ICD-10 codes associated with the original order where the ANA was the only test run on an individual specimen to remove any conflicting ICD codes with other tests.
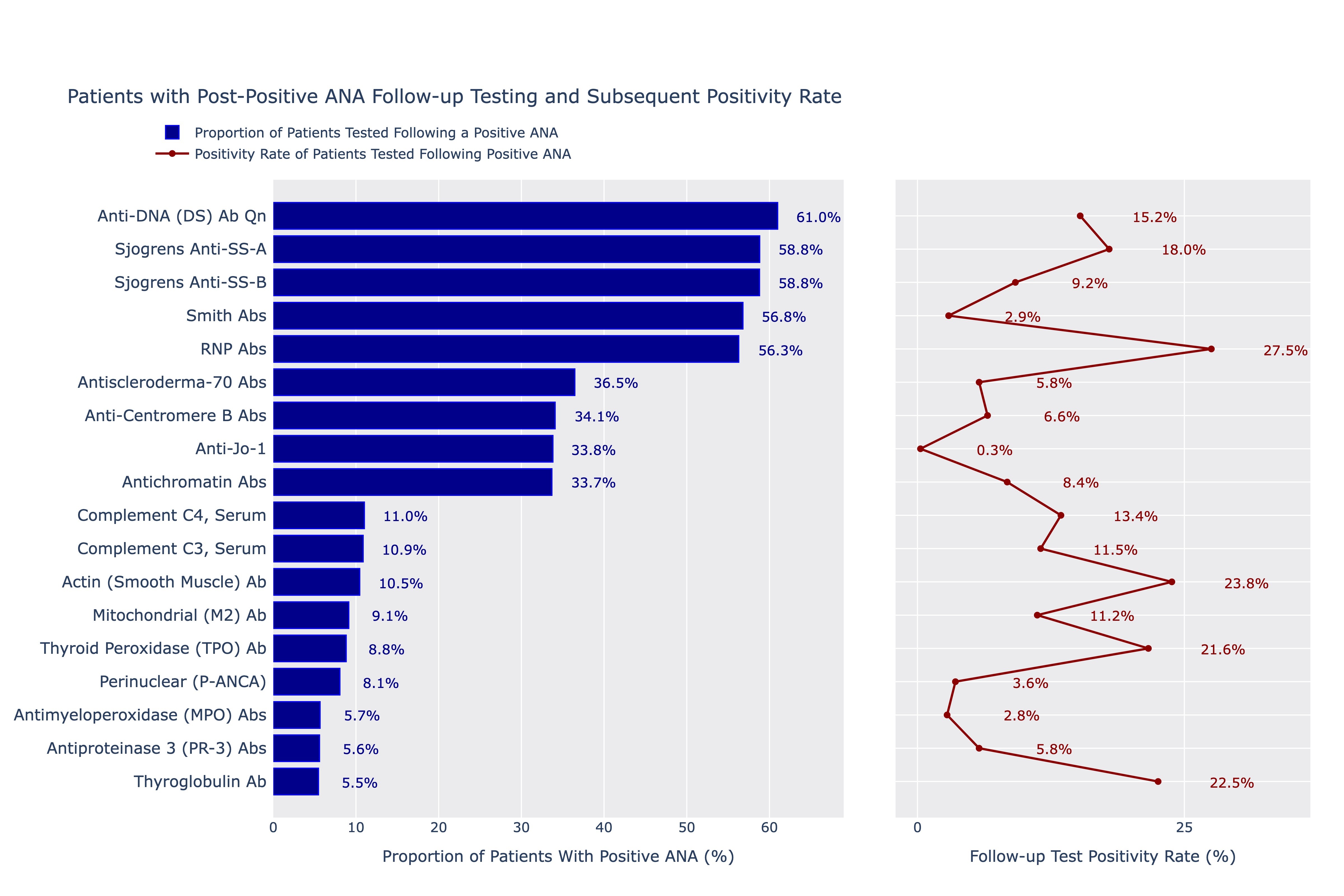
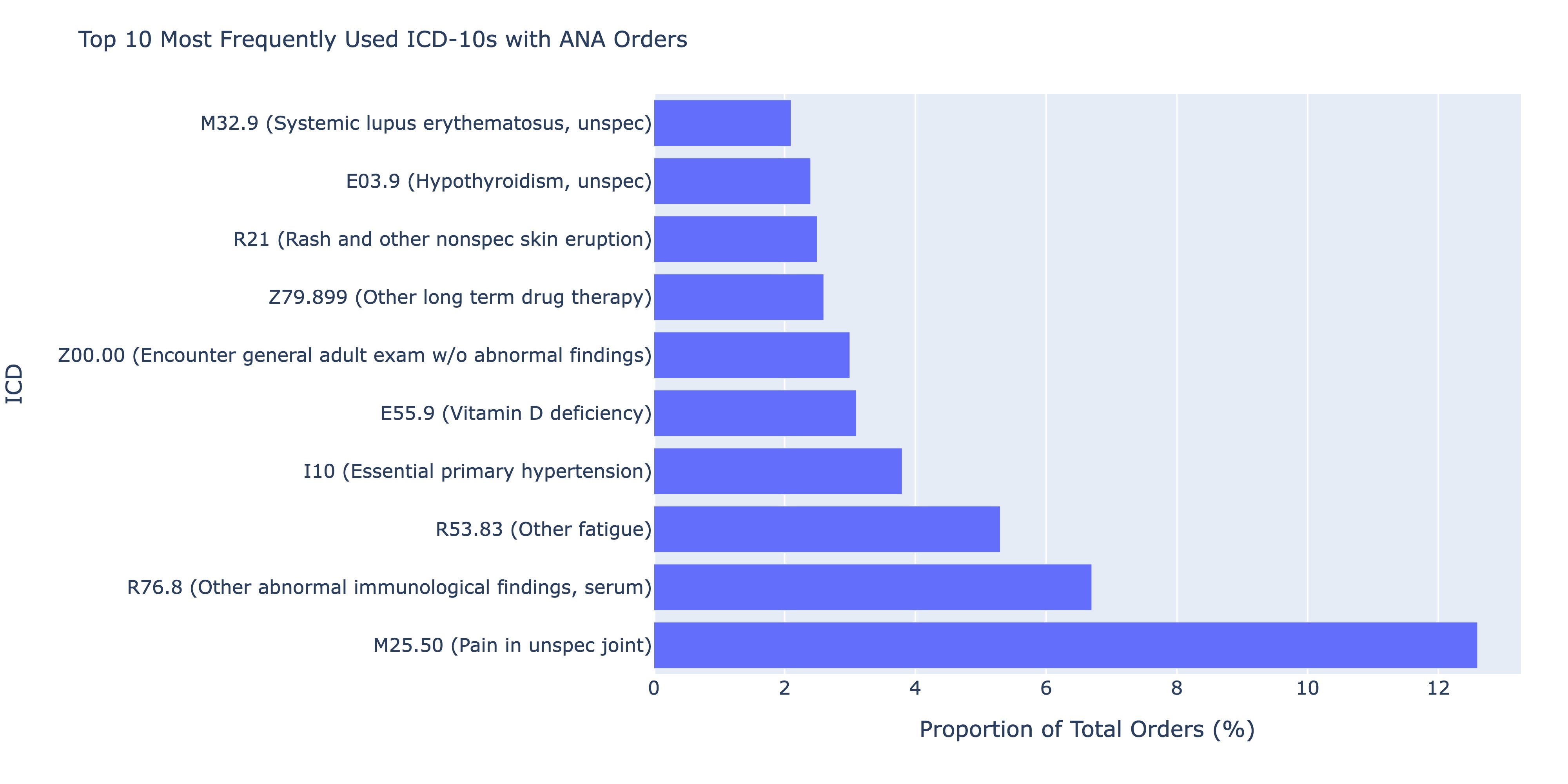
Results: A total of 1,834,048 distinct ANA tests were ordered by a non-rheumatology provider between 2011 and 2022 and had positive results. Of these tests, 49.7% (n=910,683) were ordered by primary care and only 11.2% of the total sample (n=204,608) were associated with patients who had any order placed by a rheumatologist within a year of the ANA. Anti-dsDNA, anti-SSA, anti-SSB, Smith and RNP antibodies were the most frequently ordered autoimmune-specific follow-up tests performed by non-rheumatologists, each representing just over 50% of the sample. Of these, RNP antibodies had the highest positivity rate (27.5%), and Smith antibodies the lowest (2.9%). Thyroglobulin antibodies were the least ordered tests (5.5% of cohort) but had one of the highest positivity rates (22.5%). Of specimens with only an ANA ordered (n=148,882), M25.50 (pain in unspecified joint, 12.6% of the cohort), R76.8 (other abnormal findings in serum, 6.7%) and R53.83 (other fatigue, 5.3%), I10 (essential primary hypertension, 3.8%) and E55.9 (Vitamin D deficiency, 3.1%) were the most frequent ICD-10s ordered but together represented only 8.1% of the total cohort.
Conclusion: There does not appear to be a clear ordering pattern of follow-up testing within a year of a positive ANA test. While more than half of the cohort received some common antibody tests like Anti-dsDNA, positivity rates were low. Interestingly, approximately 10% of the cohort had an order from a rheumatologist within a year, suggesting the majority of diagnostic workup is being done by primary care. Ordering ICD-10 codes represent suspicion for a rheumatologic process and symptoms, such as joint pain, but the frequency of hypertension and Vitamin D deficiency codes do not readily explain a reason for ordering. Results suggest the need for a guideline approach for rheumatologic disorder testing evaluation and education in the non-rheumatologic setting.
Patients with Post-Positive ANA Follow-up Testing and Subsequent Positivity Rate
Top 10 Most Frequently Used ICD-10s with ANA orders
D. Alfego: None; Q. Hlatky: Labcorp, 3; S. Naides: Laboratory Corporation of America Holdings (Labcorp), 3; K. Lee: None; J. Ennis: Labcorp, 3, 11; K. Clark: Labcorp, 3.