Hospital San Jose Tecnologico de Monterrey Monterrey, Nuevo Le�n, Mexico
Disclosure information not submitted.
Mario R. Garcia-Pompermayer1, Sarah G. Ayton2, Karina Silva Luna3 and Mario Alberto Garza Elizondo3, 1Hospital San Jose, TecSalud, Tecnologico de Monterrey, Monterrey, Mexico, 2Mailman School of Public Health, Columbia University, New York, NY, 3Hospital Zambrano-Hellion, TecSalud, Tecnologico de Monterrey, Monterrey, Mexico
Background/Purpose: Musculoskeletal ultrasound (MSUS) is a valuable tool in Rheumatology as it is non-invasive, cost-effective, and useful in regular clinical practice. However, its adoption has been slow and MSUS education in Mexico is limited. Our objective is to assess MSUS knowledge, attitudes, and practices in young Rheumatologists in Mexico and identify potential barriers and facilitators to its clinical use.
Methods: An online survey was distributed to ReumaJoven, a network of young Rheumatologists in Mexico. The survey captured demographics, and general, institutional, and personal MSUS information. The need for MSUS in Rheumatology in Mexico was assessed for association with knowledge, attitudes, and practices. Multivariable analysis using elastic net and bootstrapping identified drivers of respondent attitudes.
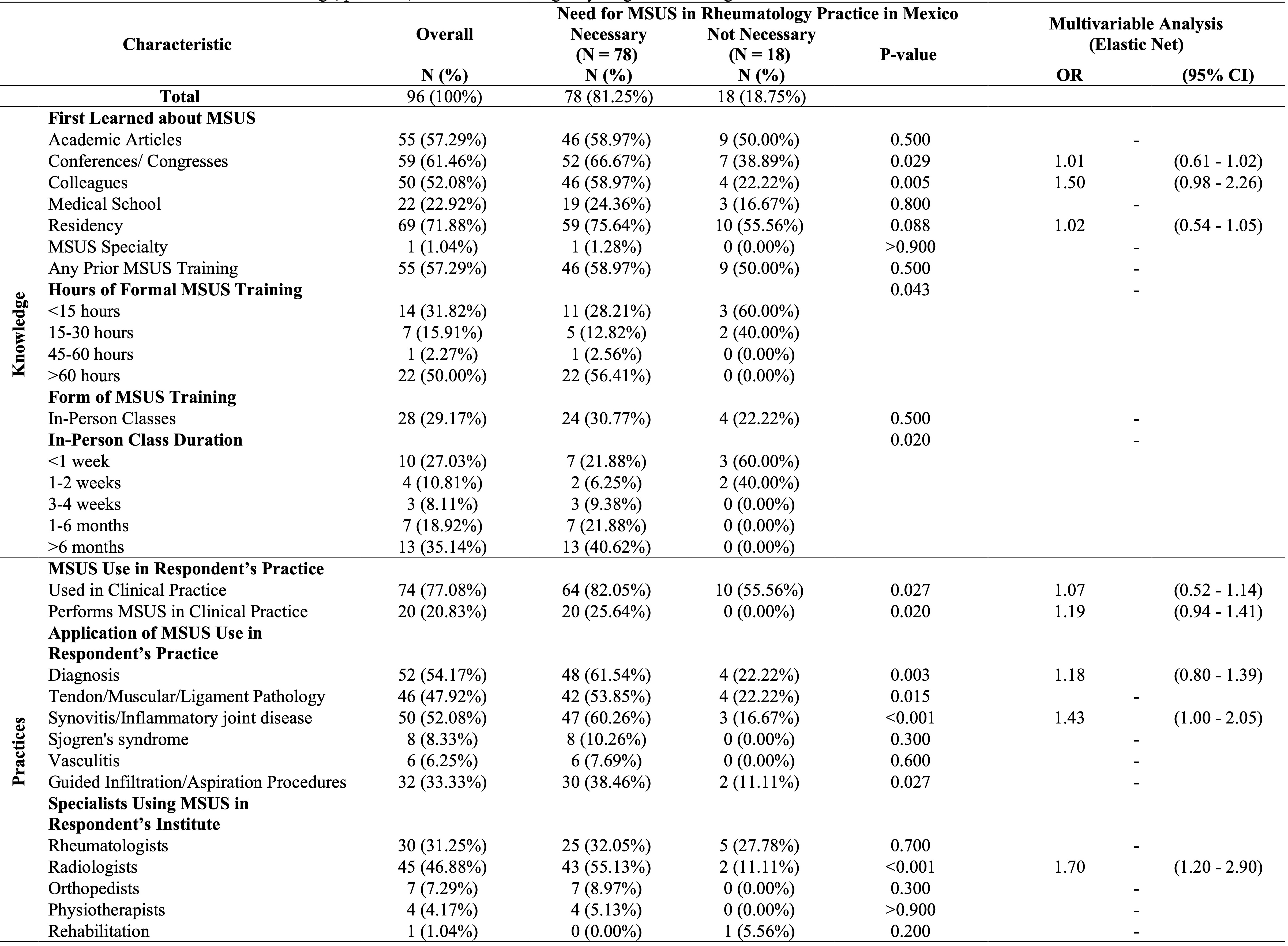
Results: Rheumatologists (n=91) completed the survey (women: n=52, 54.17%, age: median=35.08, IQR: 32.79-37.73 years). Most worked in public hospitals (n=65, 67.71%) and private practices (n=80, 83.33%), including residents (n=5, 5.21%), professors (n=37, 38.54%), and non-academic clinicians (n=54, 56.25%). The most prominent barriers to MSUS were lack of access to training (important or very important: n=54, 56.25%) and training time required (n=52, 54.17%). Lack of scientific evidence was not an important barrier to MSUS use (unimportant or very unimportant: n=58, 60.42%). Most (n=78, 81.25%) reported MSUS is necessary in clinical Rheumatology practice in Mexico. This positive MSUS attitude was significantly associated with learning about MSUS from conferences (p=0.029) and colleagues (p=0.005), formal (p=0.043) and in-person training (p=0.020), use in the respondent's practice (p=0.027), and MSUS use by Radiologists in the respondent's institute (p< 0.001). Most were interested in learning MSUS (n=85, 88.54%), which was significantly increased in those reporting positive MSUS attitudes (n=74, 94.49%, p< 0.001). Elastic net identified drivers of positive MSUS attitudes, including learning about MSUS from conferences, colleagues, and in residency; use of MSUS in the respondent's practice, the respondent performing MSUS, using MSUS for diagnosis or monitoring of Synovitis/Inflammatory joint disease; and use of MSUS by Radiologists in the respondent's institute. Use of MSUS for diagnosis or monitoring of Synovitis/Inflammatory joint disease (OR=1.43, 95%CI: 1.00-2.05) and use of MSUS by Radiologists in the respondent's institute (OR=1.70, 95%CI: 1.20-2.90) were statistically significantly associated with positive MSUS attitudes in the final multivariable analysis.
Conclusion: This study assessed knowledge, attitudes, and practices of MSUS among young Rheumatologists in Mexico and identified barriers and facilitators to its implementation. Most recognized the necessity of MSUS in clinical practice, particularly those with prior training, who used MSUS in their practice, and had access to MSUS expertise. Improving MSUS education and training opportunities, and promoting collaboration between Rheumatologists and Radiologists may overcome barriers to adoption of MSUS in Mexico, ultimately improving patient care.
Figure 1. Responses to questions about the advantages, disadvantages, interest in learning, and barriers to implementing (clockwise from top left) MSUS among young Rheumatologists in Mexico.
Table 1. Characteristics of MSUS knowledge, practices, and attitudes among 96 young Rheumatologists in Mexico.
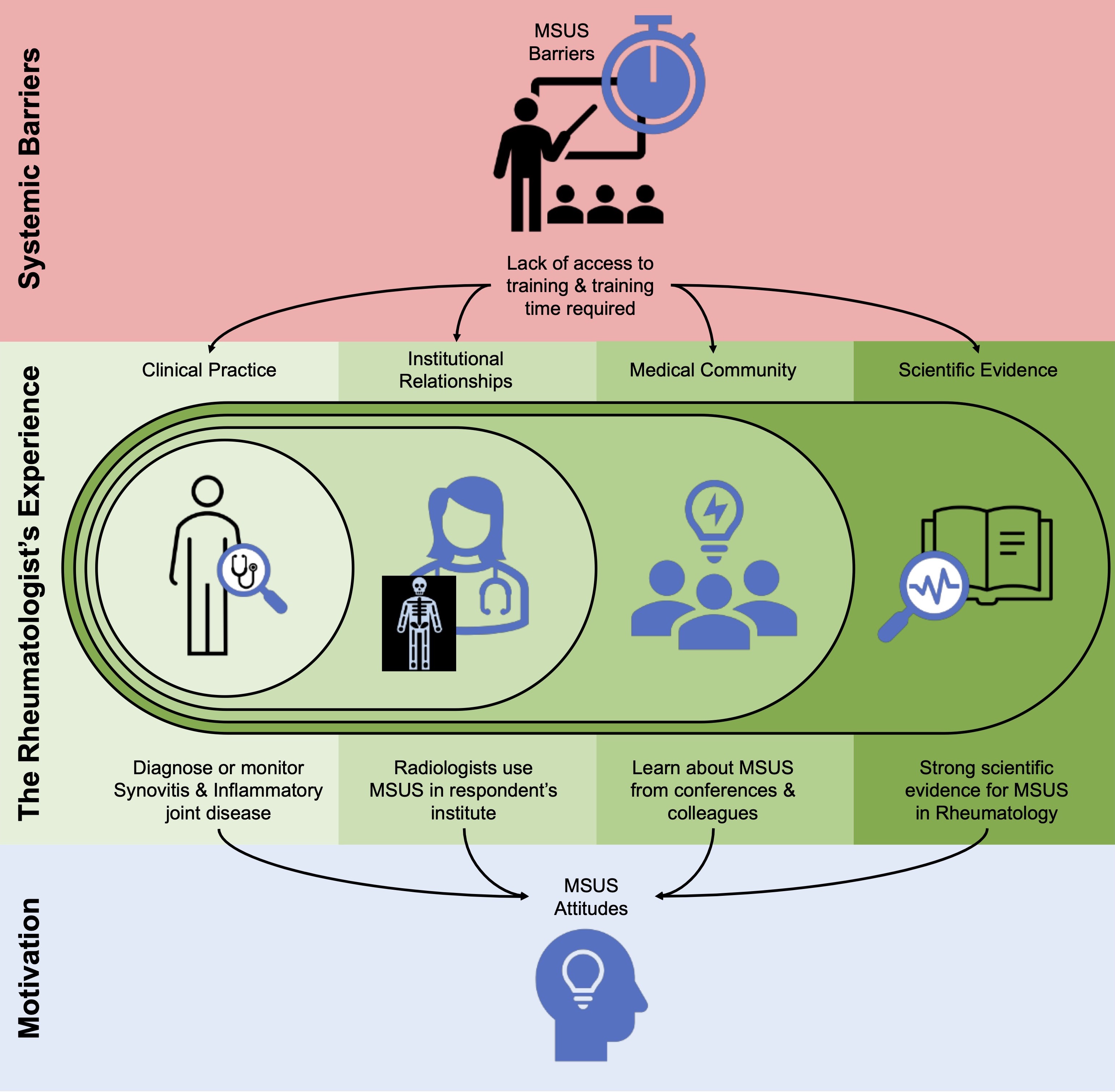
Figure 2. Overview of facilitators and barriers to implementing MSUS in clinical practice. Systemic barriers to MSUS implementation impact the Rheumatologist’s experience of their clinical practice, institutional resources, knowledge shared in the medical community, and the available scientific evidence. Notably, use of MSUS for diagnosis and monitoring synovitis and inflammatory joint disease in clinical practice, having Radiologists who use MSUS in their institute, learning about MSUS from the medical community, and the strong scientific evidence surrounding MSUS all drive positive attitudes and impact motivation to implement MSUS.
M. Garcia-Pompermayer: None; S. Ayton: None; K. Silva Luna: None; M. Garza Elizondo: None.



.jpg)