Session: (1383–1411) Spondyloarthritis Including Psoriatic Arthritis – Diagnosis, Manifestations, & Outcomes Poster II: Imaging & AS
1406: Temporal Trends in Cardiovascular Events in Axial Spondyloarthritis Patients with Medicare Insurance versus Commercial Insurance: An Analysis Using Claims Data
University of Alabama Birmingham Birmingham, AL, United States
Disclosure information not submitted.
Rouhin Sen1, Justin Leach1, Maria I. (\"Maio\") Danila2, Fenglong Xie1, Jasvinder Singh1, Liron Caplan3, Iris Navarro-Millán4 and Jeffrey Curtis1, 1University of Alabama at Birmingham, Birmingham, AL, 2University of Alabama at Birmingham (UAB), Birmingham VA Medical Center, Birmingham, AL, 3Rocky Mountain Regional VAMC, Aurora, CO, 4Weill Cornell Medicine, Hospital for Special Surgery, New York, NY
Background/Purpose: AS is an inflammatory disorder of the axial skeleton and can cause complications including disabling joint damage. Nearly 20% of people with AS are on Medicare disability insurance1. Major adverse cardiovascular events (MACE) are the leading cause of death in AS2. Despite the high prevalence of disability in AS, these patients are understudied1 and may be different than similarly aged commercially insured patients. We sought to compare MACE incidence temporal trends in AS patients who are beneficiaries of Medicare disability insurance against those with commercial insurance in order to understand the excess risk for CVD events in disabled patients.
Methods: We conducted a retrospective longitudinal analysis from 2007-2019 using the Medicare Fee-for-Service and MarketScan claims databases. Subjects were identified by having ≥ 2 AS International Classification of Diseases (ICD)-9/10 diagnosis codes in outpatient visits with age between 18 and 64 years. MACE was defined as an incident hospitalized myocardial infarction or ischemic stroke and identified by validated ICD 9/10 diagnosis codes. Patients with prior MACE were excluded3. We reported demographics, cumulative raw incidence/1000 person and determined incidence rate ratios for disabled Medicare enrollees versus commercially insured AS patients. We displayed incidence trends and calculated yearly annual percentage change (APC) based off end-of-year cutpoints; significance was determined using the Monte Carlo Permutations method. SAS v9.4 and Joinpoint Trend Analysis v5.0 software were used for analyses; p < 0.05 determined statistical significance.
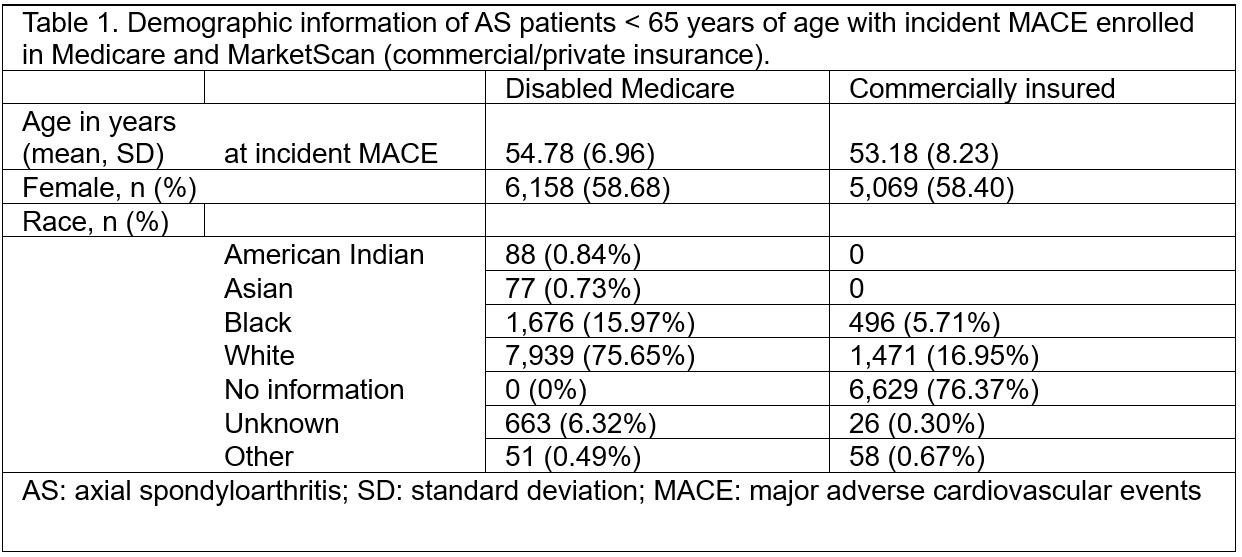
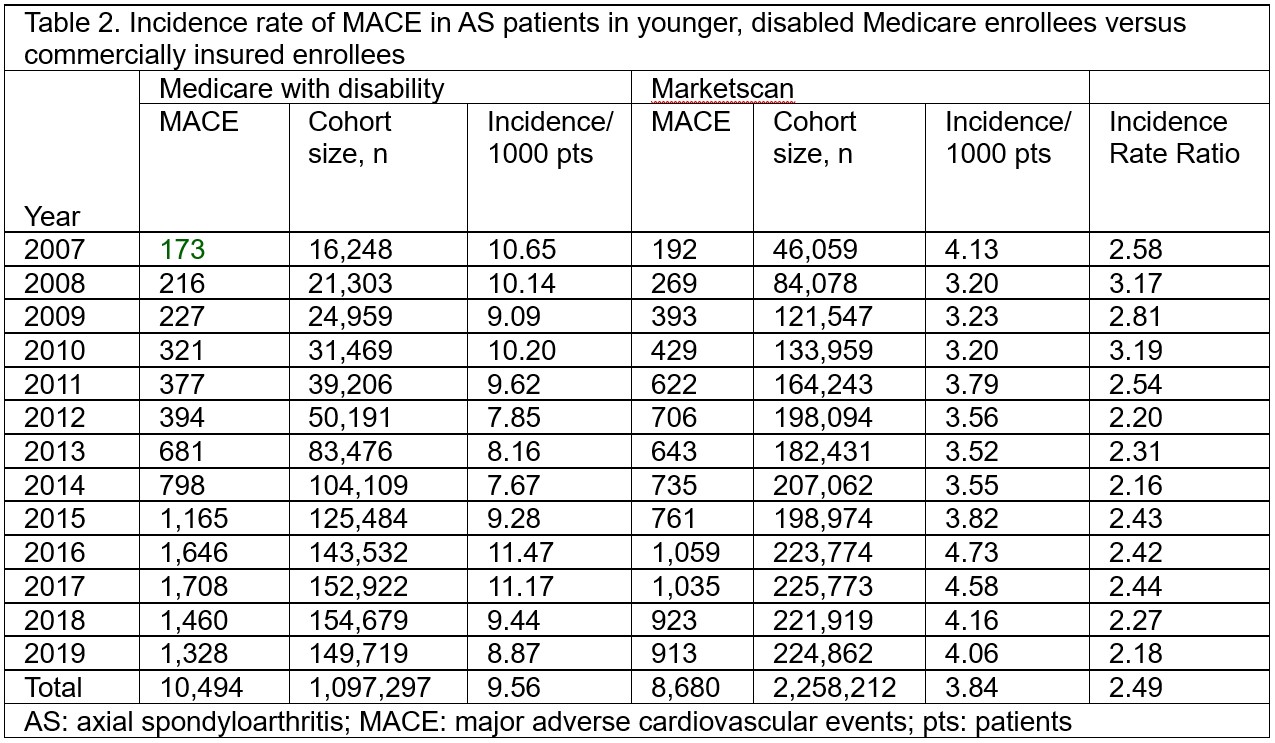
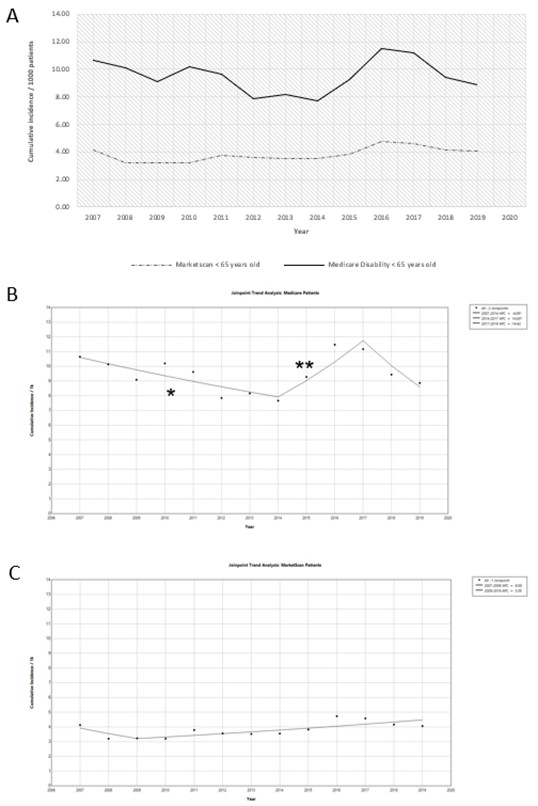
Results: The total number of AS patients eligible for analysis was 1,097,297 from Medicare and 2,258,212 from MarketScan. Incident MACE was identified in 10,494 subjects in Medicare and 8,860 individuals in MarketScan. The mean age in years at which MACE occurred was 54.8 and 53.3 in patients with Medicare and MarketScan, respectively. Most patients with MACE were female and White (Table 1). In the disabled Medicare cohort, the incidence of MACE ranged from 7.7-11.5/1000 patients. This cohort showed a significant decrease in incidence from 2007-2014 (-4.1 APC), then a significant increase from 2014-2017 (14.0 APC), then no significant difference from 2017-2019 (Figure 2b). In the MarketScan cohort, the incidence of MACE was between 3.2-4.7/1000 patients and there was a non-significant upward trend (3.4 APC) in the MACE incidence rate (Figure 1c). The incidence rate ratio compared disabled Medicare enrollees with AS to commercially insured AS patients ranged from 2.2-3 (Table 2).
Conclusion: Disabled AS patients younger than age 65 years with Medicare experienced a 2-3-fold higher incidence of MACE compared to younger commercially insured patients; unexpectedly, the group of AS patients experiencing MACE events was made up of a high percentage of women. Incidence trend for MACE differed for both groups and did show signs of increase, though not significant. Our future research is to understand why there is a difference between the groups, including differences in the prevalence comorbidities, socioeconomic status, treatment patterns, and healthcare access.
Figure 1. Incidence rate trend of Myocardial infarction and ischemic stroke in AS patients. Panel A: Raw incidence/1000 patients enrolled in Medicare (dark, solid line) versus MarketScan insurance (dashed line). Panel B: JoinPoint analysis of the raw incidence trend for Medicare patients. The single asterisk (*) displayed under the trend line shows a significant decrease in incidence (-4.09 APC) from 2007-2014 while the double asterisk (**) depicts a statistically significant increase in incidence (14.00 APC) from 2017-2019. Panel C JoinPoint analysis of the raw incidence trend for commercially or privately insured MarketScan patients. There was no statistically significant difference in the incidence trend.
R. Sen: None; J. Leach: None; M. Danila: Horizon, 5, Pfizer, 5, RheumNow, 2, UCB, 2; F. Xie: None; J. Singh: Other, 2, 6, 11, 11, 12, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics Inc., Seres Therapeutics, Tonix, Charlotte’s Web, 12, Atai life sciences, kintara therapeutics, Intelligent Biosolutions, Acumen pharmaceutical, TPT Global Tech, Vaxart pharmaceuticals, Atyu biopharma, 12, speaker’s bureau of Simply Speaking, other, 12, received institutional research support from Zimmer Biomet Holdings. JAS received food and beverage payments from Intuitive Surgical Inc./Philips Elec, Other, 12, Schipher, Crealta/Horizon, Medisys, Fidia, PK Med, Two labs Inc., Adept Field Solutions, Clinical Care options, Clearview healthcare partners, Putnam; L. Caplan: None; I. Navarro-Millán: None; J. Curtis: AbbVie, 2, 5, Amgen, 2, 5, Bristol-Myers Squibb, 2, 5, CorEvitas, 2, 5, Eli Lilly and Company, 2, 5, Janssen, 2, 5, Myriad, 2, 5, Novartis, 2, 5, Pfizer, 2, 5, Sanofi, 2, 5, UCB, 2, 5.