Session: (1383–1411) Spondyloarthritis Including Psoriatic Arthritis – Diagnosis, Manifestations, & Outcomes Poster II: Imaging & AS
1394: Comorbidities, Not Long-Term Use of Nonsteroidal Anti-Inflammatory Drugs, May Be Associated with Chronic Kidney Disease in Patients with Ankylosing Spondylitis: A Nationwide Population-Based Study
Inje University Seoul Paik Hospital Seoul, South Korea
Disclosure information not submitted.
Bon San Koo1, Subin Hwang1, Ye-Jee Kim2, Soo Min Ahn2 and Wook Jang Seo3, 1Inje University Seoul Paik Hospital, Seoul, South Korea, 2Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea, 3Department of Rheumatology, Veteran Health Service Medical Center, Seoul, South Korea
Background/Purpose: Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed as first-line treatment for symptom relief and inflammation reduction in patients with ankylosing spondylitis (AS). However, long-term NSAID use has been linked to an increased risk of developing chronic kidney disease (CKD). This study aimed to identify the risk factors, including cumulative NSAID dosage, associated with CKD in AS patients using data from the National Health Insurance.
Methods: The incidence of CKD was determined in AS patients diagnosed between May 1, 2016, and December 31, 2019, using Korean national health insurance data. The cumulative NSAID dosage was assessed using the ASAS NSAID Intake Score. The ASAS NSAID Intake Score was categorized into four groups based on the score at 3 months, 6 months, and 1-year intervals: = 0, >0 and ≤33.3, >33.3 and ≤66.6, and >66.6. The hazard ratio was used to evaluate the risk of CKD based on baseline characteristics. A nested case-control analysis was performed to investigate the correlation between the ASAS NSAID Intake Score during 3 months, 6 months, and 1 year before CKD diagnosis and the development of CKD.
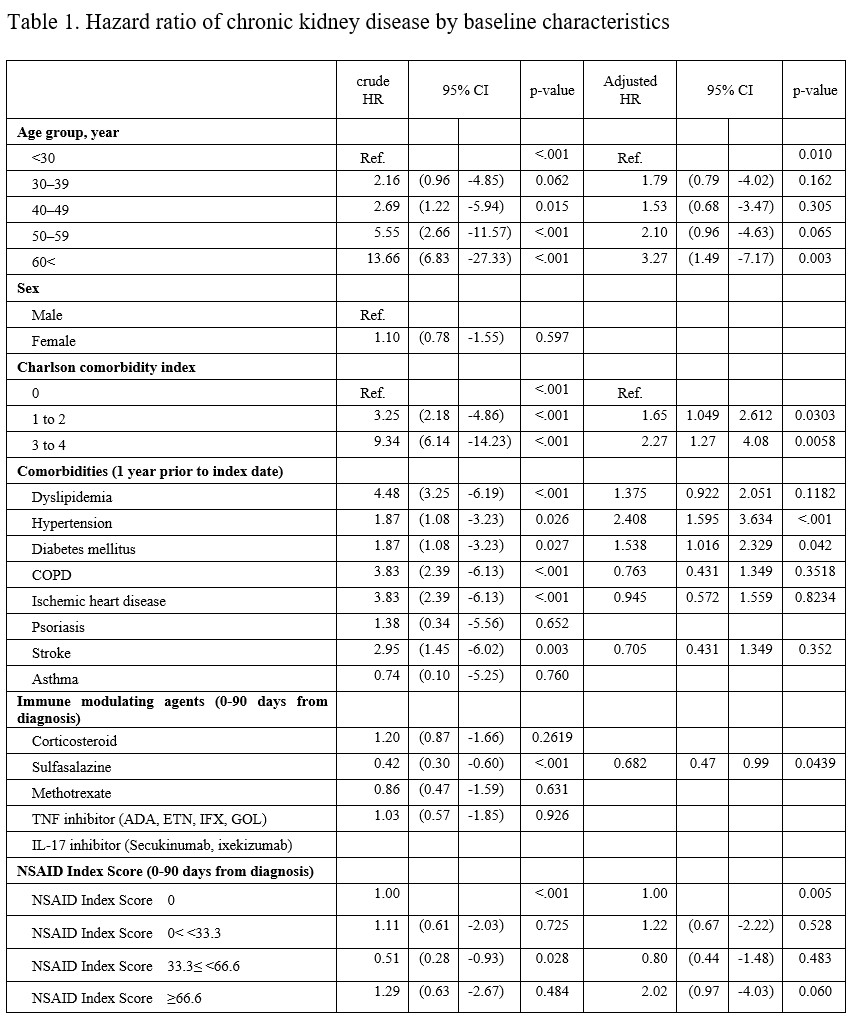
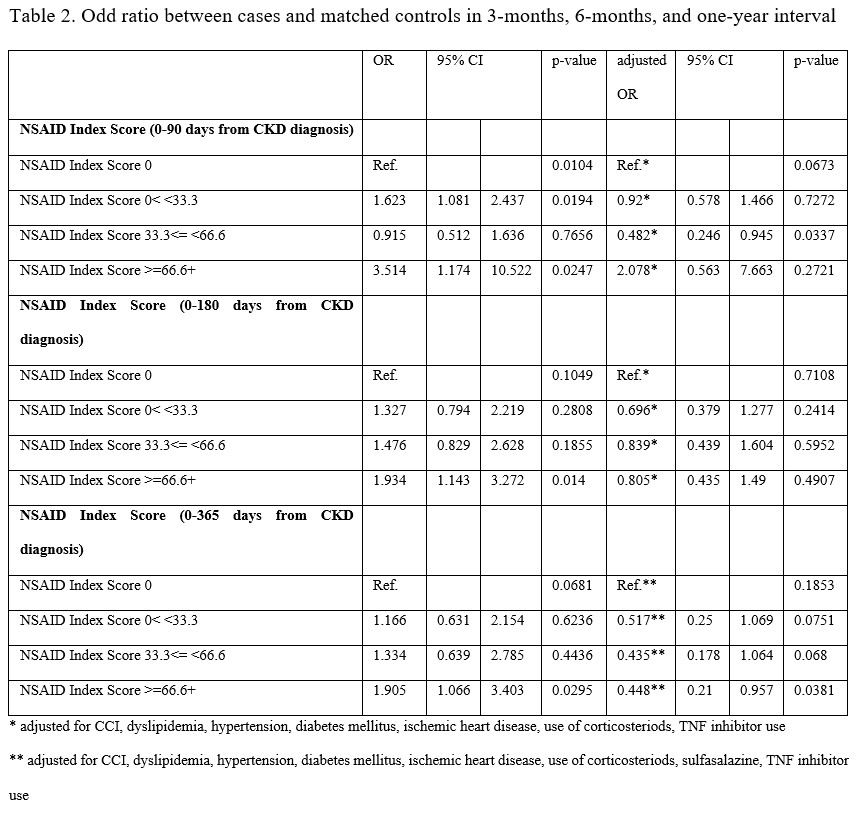
Results: Out of the initial 12,000 AS patients, 120 were identified with CKD. The incidence rate of CKD was 4.64 per 10,000 patient-years. Factors significantly associated with CKD included age ≥60 (Ref. age< 30, HR 3.27, 95% CI 1.49 – 7.17), Charlson comorbidity index 1–2 (HR 1.65, 95% CI 1.049 – 2.612) and 3–4 (HR 2.27, 95% CI 1.27 – 4.08), hypertension (HR 2.408, 95% CI 1.595 – 3.634), diabetes mellitus (HR 1.538, 95% CI 1.016 – 2.329), and sulfasalazine (HR 0.682.76, 95% CI 0.47 – 0.99) (Table 1). However, the odds ratios adjusted for comorbidity and medication did not show a correlation between the 3-month, 6-month, and 1-year ASAS NSAID Intake Scores and CKD. A 1-year ASAS NSAID Intake Score > 66.6 was associated with a reduced risk of CKD (OR 0.46, 95% CI 0.22–0.94) (Table 2).
Conclusion: The risk of CKD in AS patients was associated with comorbidities. However, long-term NSAID use may not be associated with an increased risk of CKD.
Table 1. Hazard ratio of chronic kidney disease by baseline characteristics
Table 2. Odd ratio between cases and matched controls in 3-months, 6-months, and one-year interval
B. Koo: None; S. Hwang: None; Y. Kim: None; S. Ahn: None; W. Seo: None.