Harbor-UCLA Medical Center Torrance, CA, United States
Disclosure information not submitted.
George Karpouzas1, Bianca Papotti2, Sarah Ormseth3, Marcella Palumbo4, Elizabeth Hernandez3, Maria Pia Adorni5, Francesca Zimetti2, Matthew Budoff1 and Nicoletta Ronda2, 1Harbor-UCLA Medical Center, Torrance, CA, 2University of Parma, Department of Food and Drug, Parma, Italy, 3The Lundquist Institute, Torrance, CA, 4University of Parma, Parma, Italy, 5Department of Medicine and Surgery, Unit of Neuroscience, University of Parma, Parma, Italy
Background/Purpose: The ability of serum to deliver cholesterol to cells is known as cholesterol loading capacity (CLC) and associates with foam cell formation. In rheumatoid arthritis (RA), CLC was linked to long-term cardiovascular risk as well as coronary atherosclerosis burden and vulnerable plaque composition, particularly in biologic nonusers1. The relationship between changes in CLC over time and plaque progression is unknown.
Methods: Atherosclerosis (noncalcified, partially or fully calcified plaques and coronary artery calcium [CAC] score) was evaluated with coronary computed tomography angiography in 140 patients without cardiovascular disease and reassessed in 100 after 6.9±0.4 years. Presence of 5 or more plaques in a patient and lesions rendering greater than 50% luminal stenosis were considered extensive and obstructive disease respectively. CLC was measured as intracellular cholesterol content in serum treated human THP-1 monocyte-derived macrophages with a fluorimetric assay during baseline and follow-up atherosclerosis assessments. Multivariable negative binomial and robust linear regression tested the associations between changes in CLC from baseline to follow-up and coronary plaque and CAC progression and new extensive or obstructive disease respectively.
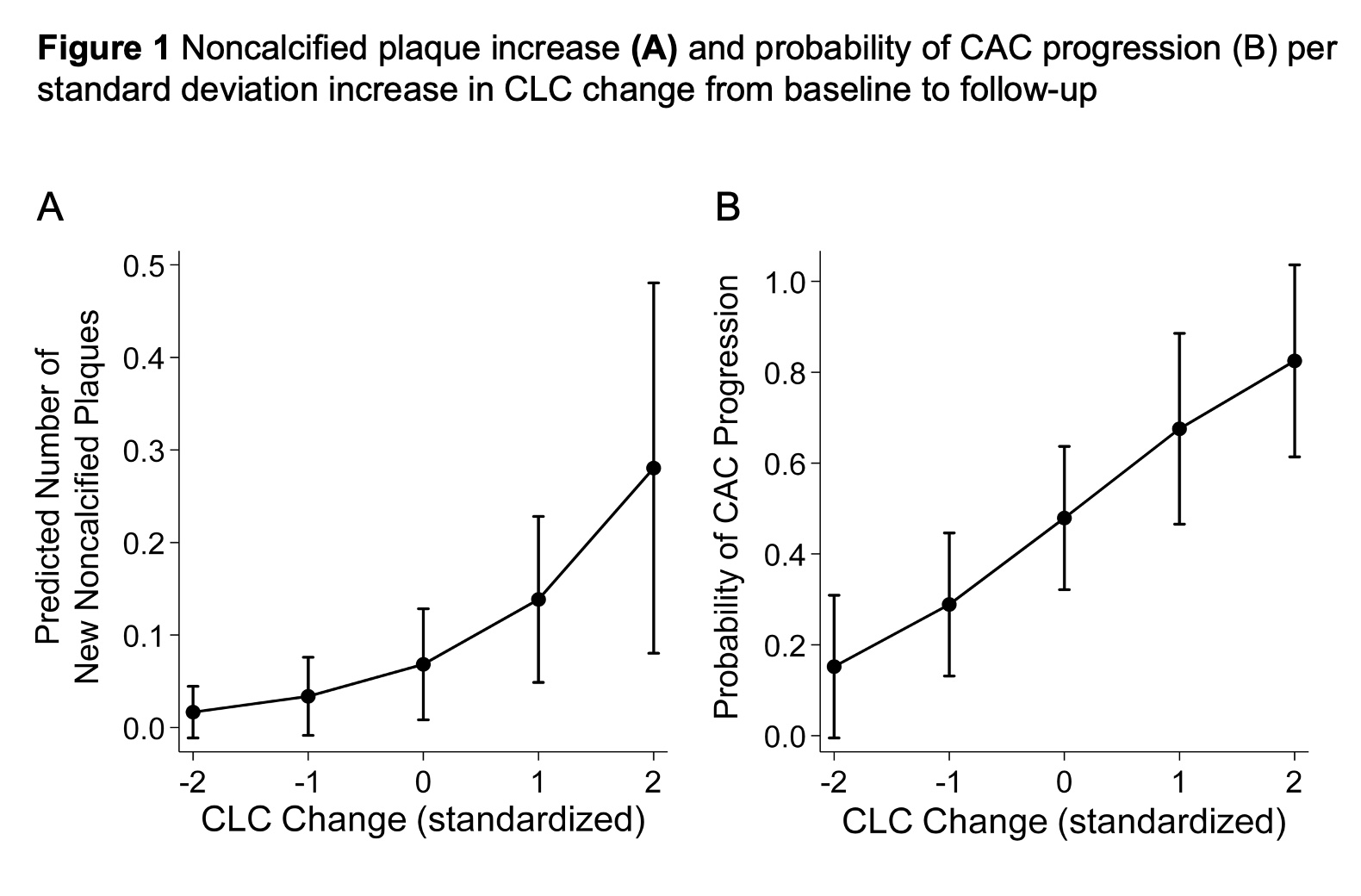
Results: CLC decreased in 68% and increased in 32% of patients at follow-up. All subjects (34/34) at the highest tertile of baseline CLC showed decrease at follow-up whereas 25/33 (75.8%) of patients at the lowest CLC tertile showed increase (p< 0.0001). CLC change (per standard deviation) associated with noncalcified plaque increase after adjusting for atherosclerotic cardiovascular disease (ASCVD) score, baseline plaque burden, obesity and duration of prednisone exposure throughout follow-up (incident rate ratio [IRR] 2.03, 95% confidence interval [95%CI] 1.27-3.24, p=0.003); risk of CAC increase after adjustments for ASCVD, baseline CAC, time-averaged c-reactive protein (TA-CRP), weighted daily-average atorvastatin equivalent dose and obesity (odds ratio [OR] 2.26, 95%CI 1.25-3.24, p=0.007) and risk of new extensive or obstructive disease at follow-up after adjusting for ASCVD, baseline plaque and TA-CRP (OR 3.17, 95%CI 1.01-9.94, p=0.048). Incrementally higher CLC at follow-up compared to baseline associated with progressively more new noncalcified plaques, greater risk of CAC increase and new extensive or obstructive disease. In contrast, greater decreases in follow-up CLC associated with significantly fewer new noncalcified plaques (Figure 1A), gradually lower risk of CAC increase (Figure 1B) and new extensive or obstructive disease.
Conclusion: Increasing CLC and therefore rising cholesterol content in arterial wall macrophages over time associates with coronary atherosclerosis progression in a dose-dependent manner, and particularly higher burden of lipid rich noncalcified plaques and extensive or obstructive disease conveying the greatest cardiovascular risk.
1Karpouzas GA et al. RMD Open 2022;8:e002411
G. Karpouzas: Janssen, 1, Pfizer, 5, Scipher, 1; B. Papotti: None; S. Ormseth: None; M. Palumbo: None; E. Hernandez: None; M. Adorni: None; F. Zimetti: None; M. Budoff: None; N. Ronda: None.



 photo")