Dubai Health Authority Dubai, United Arab Emirates
Disclosure information not submitted.
Jamal Al-Saleh1, Faisal Elbadawi1, Rajaie Namas2, Samar Al-Emadi3, Khalid A. Alnaqbi4, Humaid A. Al-Wahshi5, Amjad Alkadi6, Suad Hannawi7, Mohamed Hamouda8, Averyan Vasylyev8, Arwa Al-Shujairi8, Reem Al-Jayyousi9 and Munther Khamashta8, 1Dubai Hospital, Department of Rheumatology, Dubai, United Arab Emirates, 2Cleveland Clinic Abu Dhabi, Department of Rheumatology, Abu Dhabi, United Arab Emirates, 3Hamad Medical Corporation, Department of Rheumatology, Doha, Qatar, 4Tawam Hospital, Department of Rheumatology, Al Ain, United Arab Emirates, 5The Royal Hospital, Department of Rheumatology, Muscat, Oman, 6Ministry of Health, Kuwait, Kuwait, 7Kuwait Hospital, Department of Rheumatology, Dubai, United Arab Emirates, 8GSK Gulf, Medical Affairs Department, Dubai, United Arab Emirates, 9Mohamed Bin Rashid University of Medicine and Health Sciences, College of Medicine, Dubai, United Arab Emirates, and Mediclinic Parkview, Dubai, United Arab Emirates
Background/Purpose: Data from limited studies of LN in the Gulf region suggest that LN manifests more severely in this region than in Caucasian populations, yet there are no treatment recommendations specific to the Gulf region.1 This study aims to characterize patients with LN in the Gulf region to better understand disease burden and inform treatment recommendations to improve patient outcomes.
Methods: In this prospective, multicenter study (GSK Study 216989), adults with an established diagnosis of LN (biopsy proven or clinician diagnosis) were enrolled from sites in Kuwait, Oman, Qatar, and the UAE. At enrollment, the site physician extracted patient demographics and clinical characteristics retrospectively from medical charts for the previous < 12 months, and patients completed the 36-Item Short Form Health Survey (SF-36). Prospective medical chart follow-up continued for up to 12 months after enrollment. This analysis reports only data collected retrospectively at enrollment.
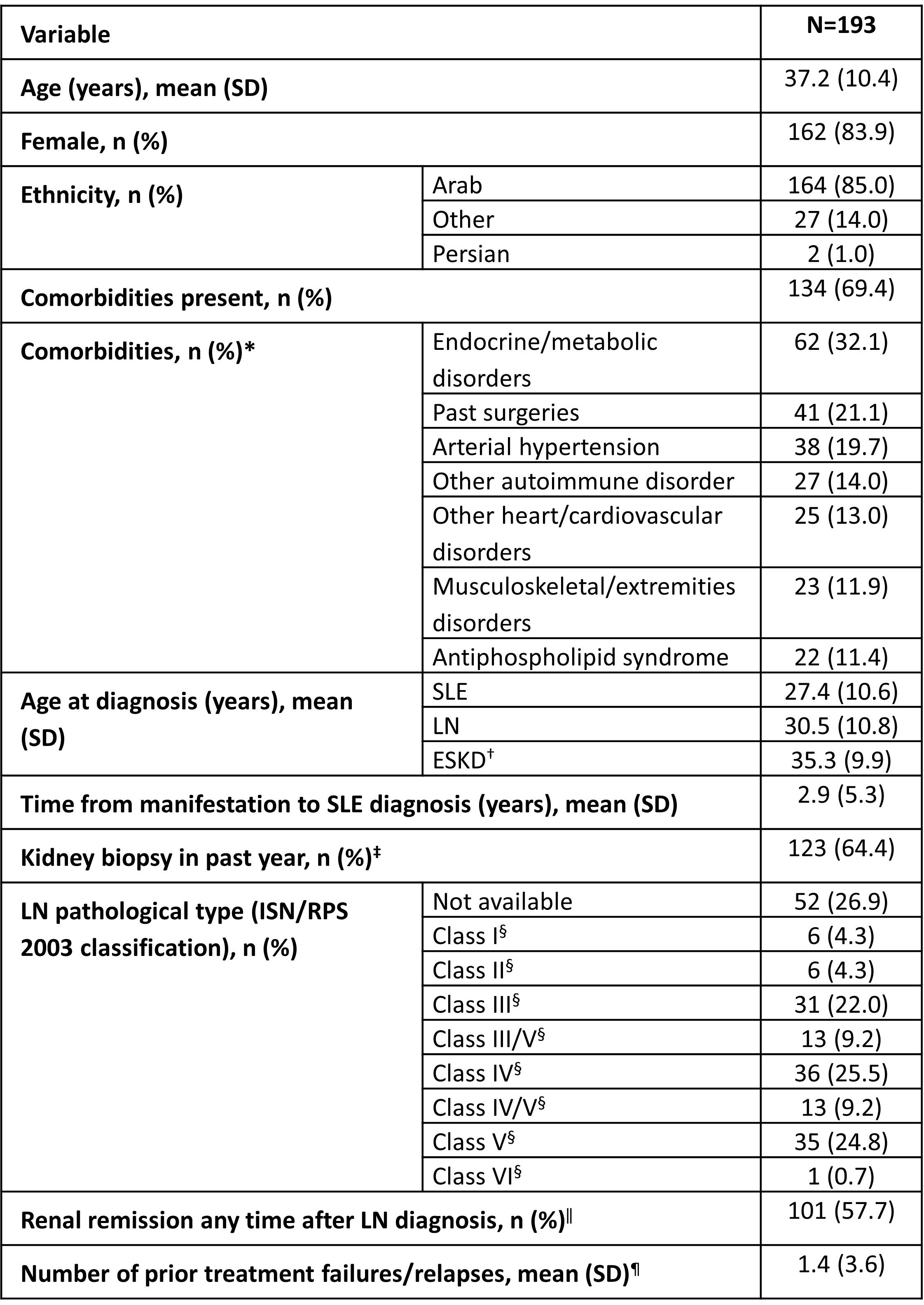
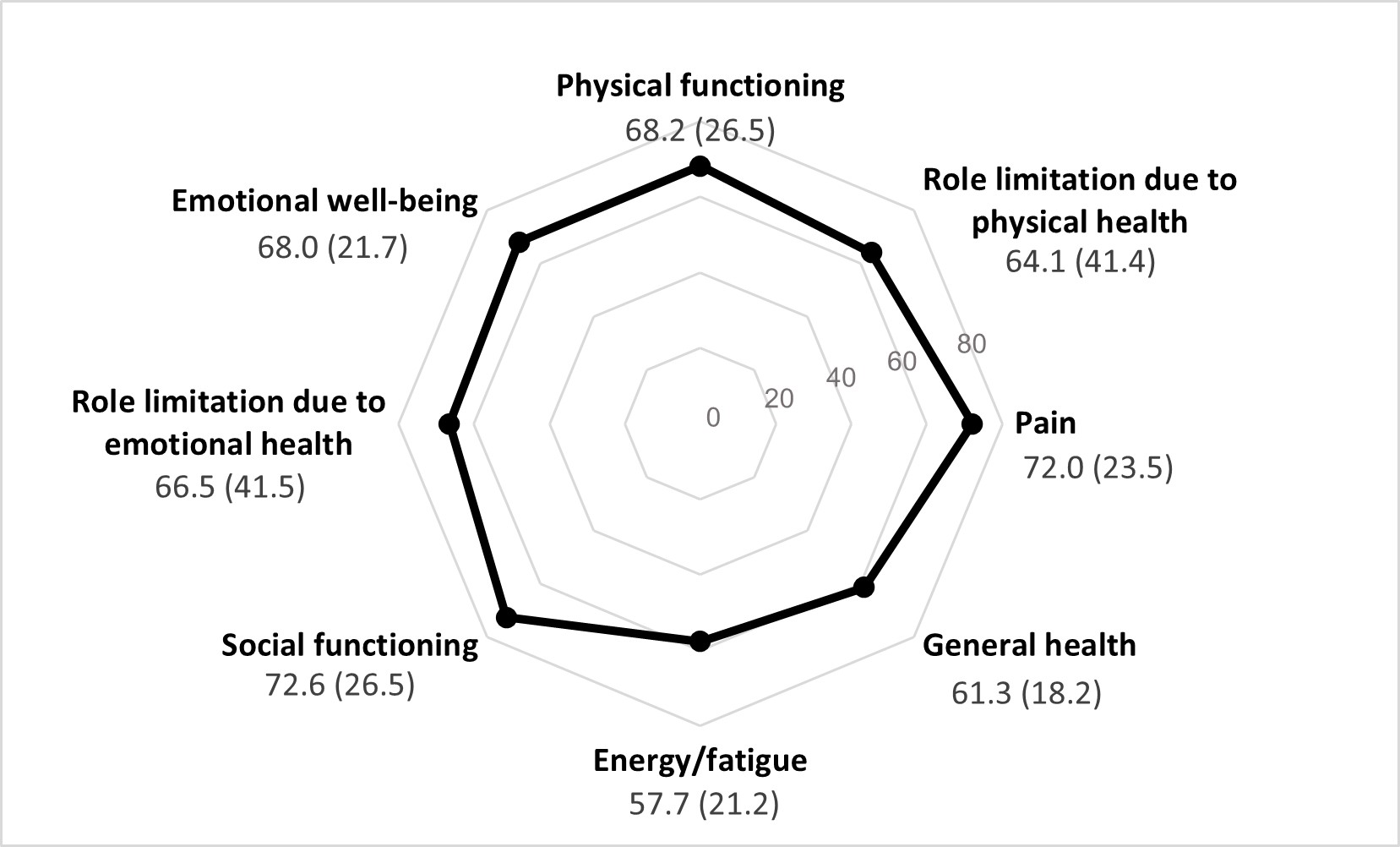
Results: This analysis comprised 193 patients with LN, the majority of whom were female (83.9%), of Arab ethnicity (85.0%), and with a mean (standard deviation [SD]) age of 37.2 (10.4) years (Table). Patients had a mean (SD) age of 27.4 (10.6) years at the time of SLE diagnosis, 30.5 (10.8) at LN diagnosis, and 35.3 (9.9) at ESKD diagnosis (n=11). Comorbidities were reported for 69.4% (n=134) of patients, most commonly endocrine and metabolic disorders (32.1%; n=62). One-third of patients had no kidney biopsy in the year preceding enrollment (35.6%; n=68), and LN class was not available for 26.9% (n=52) of patients, suggesting a potential lack of routine biopsy for some patients. Among available data, the proportions of LN Class III, IV, and V were similar (22.0–25.5%; n=31–36). Renal remission was achieved any time after LN diagnosis in 57.7% (n=101) of patients with available data. The mean (SD) number of prior treatment failures/relapses was 1.4 (3.6) in those with available data. Mean (SD) overall SF-36 score was 66.3 (19.1); scores across domains were generally similar, with energy/fatigue having the lowest score (57.7 [21.2]), and social functioning the highest (72.6 [26.5]; Figure).
Conclusion: These retrospective data suggest that approximately one-quarter of patients with LN in the Gulf region did not have sufficient histological classification to guide therapy, and these inconsistencies in histological data make it difficult to compare Gulf patient characteristics to published data from international cohorts. However, age at SLE diagnosis was young, and patients appeared to be similarly impacted across all SF-36 quality of life subscales, whereas a large international inception cohort reported relatively greater impacts in role of physical functioning than other domains.2 Prospective data generated from this cohort may aid understanding of differences in care and may have the potential to inform LN treatment guideline development in the Gulf region.
Funding: GSK
References
Al-Shujairi A et al. Lupus 2023;32:155–65
Hanly JG et al. Rheumatology (Oxford) 2016;55(2):252–62
Table. Summary of demographics and characteristics among patients with LN in the Gulf region.
*Those reported for >10% of patients are shown; †for 11 of the 12 patients with ESKD; ‡percentage among those with available data (n=191); §percentage among those with classification (n=141) ‖percentage among those with available data (n=175); ¶data missing for 42 patients (n=151). ISN/RPS, International Society of Nephrology and the Renal Pathology Society.
Figure. Mean (SD) SF-36 subscale scores (N=193).
J. Al-Saleh: Dubai Academic Health Service, 3, Sheikh Hamdan, 5; F. Elbadawi: GSK, 2; R. Namas: None; S. Al-Emadi: AbbVie, 2, 6, AstraZeneca, 2, 6, Johnson & Johnson, 2, 6; K. Alnaqbi: Tawam Hospital, SEHA Abu Dhabi, 3; H. Al-Wahshi: GSK, 2, Ministry of Health, Oman, 3; A. Alkadi: Sabah hospital-ministry of health-Kuwait, 3; S. Hannawi: GSK, 2, 6; M. Hamouda: GSK, 3; A. Vasylyev: GSK, 3, 11; A. Al-Shujairi: GSK, 3; R. Al-Jayyousi: GSK, 2, 6; M. Khamashta: GSK, 3, 11.