Session: (1442–1487) SLE – Diagnosis, Manifestations, & Outcomes Poster II
1462: Cardiovascular Damage in Systemic Lupus Erythematosus Occurs at Early Stages of the Disease. Chronological Analysis of Damage Accrual in a Large Cohort from the Spanish Society of Rheumatology Lupus Registry (RELESSER)
Complejo Hospitalario Universitario de Vigo Vigo, Spain
Disclosure information not submitted.
Sara garcia Perez1, Jose-Maria Pego-Reigosa2, Irene Altabás González1, Norman Jiménez3, Victor Del campo Perez4, JULIA MARTINEZ BARRIO5, Maria Galindo-Izquierdo6, Jaime Calvo- Alén7, Esther Uriarte Isacelaya8, Eva Tomero Muriel9, Mercedes Freire González10, Victor Martinez-Taboada11, Paloma Vela12, Antonio Fernandez-Nebro13, Alejandro Olivé-Marqués14, Javier Narvaez15, Raúl Menor-Almagro16, Gregorio Santos Soler17, José Ángel Hernández Beriain18, Javier Manero ruiz19, Elena Aurrecoechea Aguinaga20, Oihane Ibarguengoitia-Barrena21, Carlos Montilla-Morales22, Gema Bonilla23, Vicente Torrente-Segarra24, Ana Paula Cacheda25, Maria J. García-Villanueva26, Clara Moriano Morales27, Concepción Fito Manteca28, Cristina Bohórquez29, Nuria Lozano Rivas30 and Iñigo Rúa-Figueroa31, 1Department of Rheumatology, University Hospital of Vigo. IRIDIS Group (Investigation in Rheumatology and Immune-Diseases), Vigo, Spain, 2Rheumatology, Hospital do Meixoeiro, Vigo, Spain, 3IIRIDIS (Investigation in Rheumatology and Immune-Mediated Diseases) Group, Galicia Sur Health Research Institute., Vigo, Spain, 4Department of Epidemiology, University Hospital of Vigo, IRIDIS Group (Investigation in Rheumatology and Immune-Diseases), Vigo, Spain, 5Rheumatology, Gregorio Marañon University Hospital, Madrid, Spain, 6Rheumatology, University Hospital of 12 de Octubre, Madrid, Spain, 7Rheumatology, Bioaraba Research Unit, Hospital Universitario Araba, Vitoria, Spain, 8Rheumatology, University Hospital of Donosti, San Sebastián, Spain, 9Rheumatology, Hospital La Princesa, Madrid, Spain, 10Rheumatology department, Complexo Hospitalario Universitario A Coruña (CHUAC). Instituto de Investigación Biomédica A Coruña (INIBIC), A Coruña, Spain, 11Rheumatology, Hospital Marqués de Valdecilla, Santander, Spain, 12Department of Rheumatology, University Hospital of Alicante, Alicante, Spain, 13Hospital Regional Universitario de Málaga, Malaga, Spain, 14Department of Rheumatology, Hospital Germans Trias i Pujol, Badalona, Spain, 15Hospital Universitario de Bellvitge, Barcelona, Spain, 16Rheumatology, Hospital Jerez, Puerto De Santa María, Spain, 17Rheumatology, Hospital Marina Baixa Villajoyosa, Alicante, Spain, 18Rheumatology, Hospital Insular de Gran Canaria, Las Palmas de Gran Canaria, Spain, 19Department of Rheumatology, Hospital Universitario Miguel Servet, Zaragoza, Spain, 20Department of Rheumatology, Hospital Sierrallana, Torrelavega, Spain, 21Galdakao-Usansolo University Hospital, Bilbao, Spain, 22Rheumatology, University Hospital of Salamanca, Salamanca, Spain, 23Department of Rheumatology, Hospital Clínico Universitario La Paz, Madrid, Spain, 24Department of Rheumatology, Hospital de Sant Joan Despí Moises Broggi,, Sant Joan Despí, Spain, 25Department of Rheumatology, Hospital Son Llatzer, Palma de Mallorca, Spain, 26Hospital Ramón y Cajal, Madrid, Spain, 27Rheumatology, Hospital Universitario de León, León, Spain, 28Department of Rheumatology, University Hospital of Navarra, Pamplona, Spain, 29Department of Rheumatology, University Hospital Príncipe de Asturias, Alcalá de Henares, Spain, 30Department of Rheumatology, Hospital Clínico Universitario Virgen de la Arrixaca, Murcia, Spain, 31Rheumatology, Hospital de Gran Canaria Doctor Negrin, Las Palmas de Gran Canaria, Spain
Background/Purpose: Systemic Lupus Erythematosus (SLE) survival has improved during recent decades, so other outcomes like damage accrual become more relevant. Damage represents that clinical feature that is irreversible and occurs after SLE diagnosis, being present fot at least 6 months. Our approach is to assess damage accrual, with emphasis on the cardiovascular domain over the different stages of the disease in a large SLE cohort.
Methods: Multicentre, cross-sectional study of a cohort of 4,219 SLE patients enrolled in the Spanish Society of Rheumatology Lupus Registry (RELESSER) with an average age at diagnosis (±SD) of 35.9 (±15.1) years, 89,6% of women, 92% caucasian and the average duration (±SD) of SLE 133.2 months. Organ damage was ascertained using the SDI (SLICC/ACR Damage Index). For the chronological analysis we considered, globally and for every SDI domain, only those 1,299 patients whose dates of damage events had been recorded.
Results: After 133 months of follow-up, 2,116 (50.1%) of 4,219 patients manifested some damage. Table 1 shows the comparison between patients with and without damage in the RELESSER Cohort . The damage accrual rate was higher during early stages of the disease, with 22.0% and 38.1% of those patients accumulating damage during the first and third year after SLE diagnosis, respectively. Figure 1 graphically represents the cumulative incidence of global damage over the course of the disease.
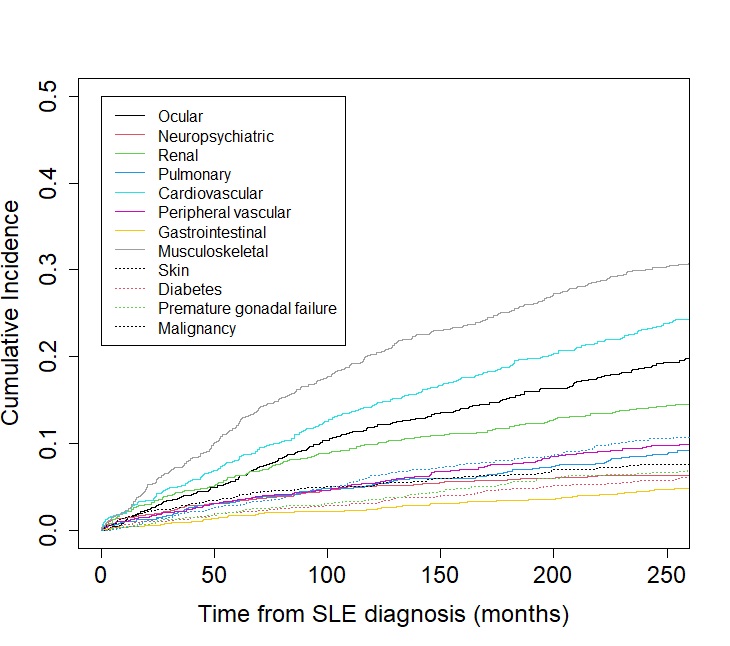
Analyzing the different domains, musculoskeletal and neuropsychiatric systems were the ones accumulating more damage at those time points. The musculoskeletal system was the one contributing more to damage during late stages.Including "cerebrovascular accident" and "claudication for 6 months" as cardiovascular items, the cardiovascular system became the second one that contributed the most to damage accrual in the early stages of SLE, with 7.0% and 11,1% of the patients who presented damage doing so in this system at year 1 and 3 after diagnosis, respectively. Figure 2 shows the cumulative incidence of damage (per SDI domain) over the course of the disease from the time of SLE diagnosis.
Conclusion: The higher rate of damage accrual occurs during the first year after SLE diagnosis. The cardiovascular system is the second leading cause of damage accrual within the first years. Strategies to prevent cardiovascular damage should be implemented early on starting from the initial SLE diagnosis.
Table 1. Comparison of patient characteristics with and without damage in the RELESSER-TRANS Cohort
Figure 1.Gobal damage over time
Figure 2. Damage over time by SDI domain
S. garcia Perez: None; J. Pego-Reigosa: None; I. Altabás González: None; N. Jiménez: None; V. Del campo Perez: None; J. MARTINEZ BARRIO: None; M. Galindo-Izquierdo: None; J. Calvo- Alén: AbbVie, 2, AstraZeneca, 2, Biogen, 6, BMS, 5, Galapagos, 6, GSK, 2, 6, Lilly, 2, 6, Novartis, 2, 6, Roche, 5, Sanofi, 2; E. Uriarte Isacelaya: None; E. Tomero Muriel: None; M. Freire González: None; V. Martinez-Taboada: None; P. Vela: None; A. Fernandez-Nebro: None; A. Olivé-Marqués: None; J. Narvaez: None; R. Menor-Almagro: None; G. Santos Soler: None; J. Hernández Beriain: None; J. Manero ruiz: None; E. Aurrecoechea Aguinaga: None; O. Ibarguengoitia-Barrena: None; C. Montilla-Morales: None; G. Bonilla: None; V. Torrente-Segarra: None; A. Cacheda: None; M. García-Villanueva: AstraZeneca, 6, GSK, 6, Otsuka, 1; C. Moriano Morales: None; C. Fito Manteca: None; C. Bohórquez: None; N. Lozano Rivas: None; I. Rúa-Figueroa: AstraZeneca, 5, GSK, 1, 6.



.jpg)
.jpg)