Amanda Steiman1, Taucha Inrig2, Katie Lundon3, Jocelyne Murdoch4 and Rachel Shupak5, 1Sinai Health System, Toronto, ON, Canada, 2St. Michael's Hospital, Toronto, ON, Canada, 3University of Toronto, Toronto, ON, Canada, 4Arthritis Society, Toronto, ON, Canada, 5St. Michael's Hospital/University of Toronto, Toronto, ON, Canada
Background/Purpose: A shortage of Rheumatologists has led to gaps in inflammatory arthritis (IA) care in Canada. Amplified in rural-remote communities, the number of Rheumatologists practicing rurally cannot be meaningfully increased. Alternate care strategies must be adopted. In this retrospective chart review, we describe the impact of a shared-care Telerheumatology model, utilizing a community-embedded Advanced Clinician Practitioner in Arthritis Care (ACPAC)-ERP and an urban-based academic Rheumatologist.
Methods: A Rheumatologist and an ACPAC-ERP established a monthly half-day Hub-and-Spoke-Telerheumatology clinic to care for patients with suspected IA, triaged by the ACPAC-ERP. Comprehensive initial assessments were conducted in-person by the ACPAC-ERP (Spoke);investigations were completed prior to the Telerheumatology visit. Retrospective analysis of demographics, time-to-key-care-indicies, patient-reported outcomes, clinical data, and estimated travel savings was performed.
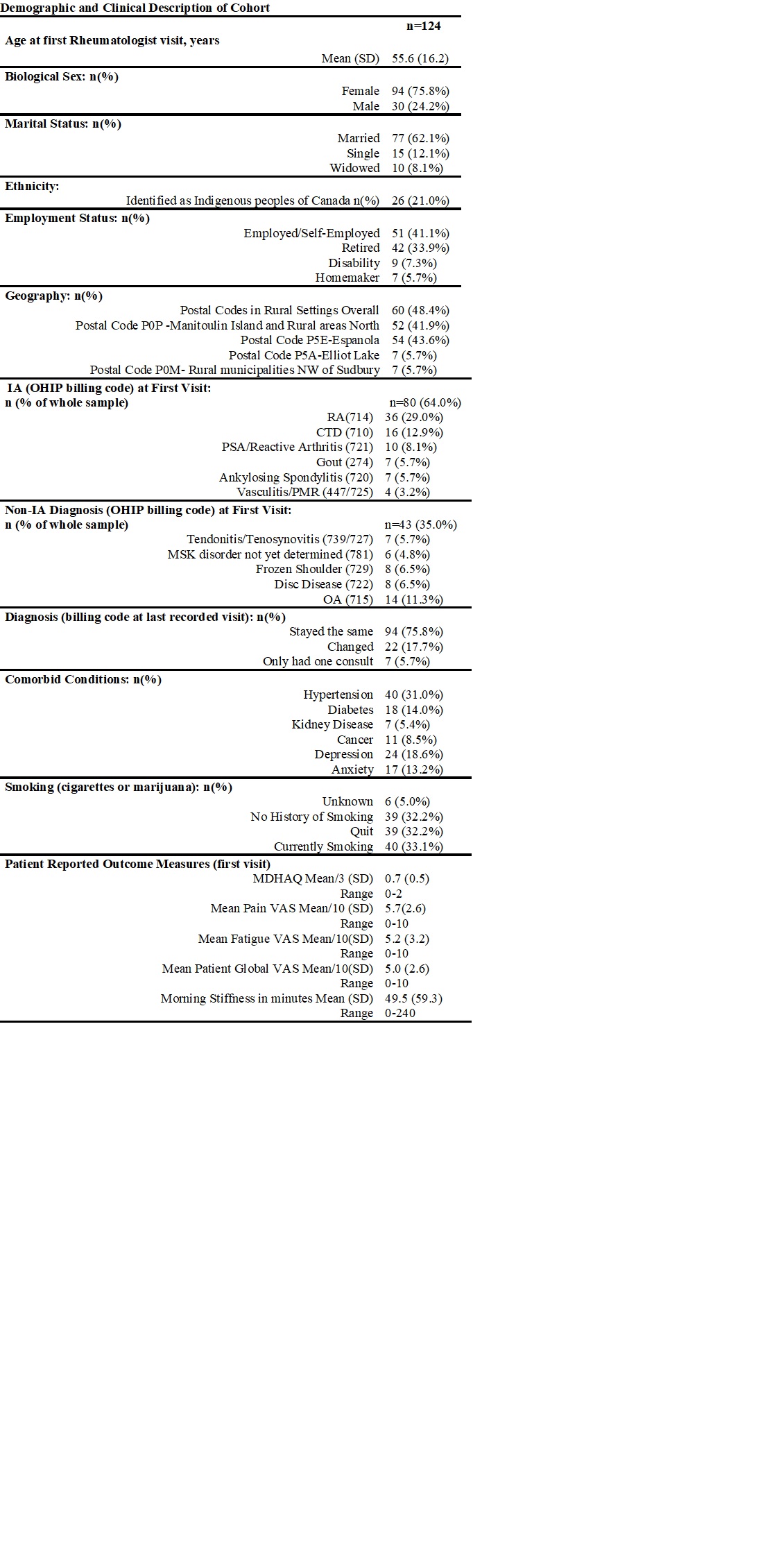
Results: Data from 124 patients seen between January 2013-January 2022 were collected: 98% (n=496/504 visits) were virtual. Average age at first visit was 55.6 years, 75% were female. IA/Connective Tissue Disease (CTD) disease was confirmed in 80/124 (64.5%) patients. Mean time from primary care referral to ACPAC-ERP assessment was52.5 days and mean time from ACPAC-ERP assessment to the Telerheumatology visit was 64.5 days. An estimated 493,470 kilometers of patient-related travel was avoided.
Conclusion: A feasible, equitable, and effective ACPAC-ERP (Spoke) and Rheumatologist (Hub) Telerheumatology model of care assessing and managing patients with suspected IA in rural/remote Ontario was described. This model can be leveraged to increase capacity to deliver comprehensive virtual rheumatologic care in underserviced communities.
Table 1: Demographics and Clinical Characteristics of Cohort
Table 2: referral, Assessment and Follow-up visits Some patients presented at first clinic visit alrady on DMARDS; of 21 who were eligible for new DMARD thrapy, treatment commenced on average in 52 days.
Figure 1: North East LHIN-based Study Population Accessing Health Services via Shared-Care Telerheumatology Model
A. Steiman: AstraZeneca, 1, GlaxoSmithKlein(GSK), 6, Pfizer, 5; T. Inrig: Pfizer, 12, I was hired by Unity Health as a Research Coordinator, my salary was supported by a Pfizer unrestricted investigator-initiated grant; K. Lundon: None; J. Murdoch: None; R. Shupak: None.



.jpg)
.jpg)
