Maria Luz Garcia Vivar1, elena abad plou2, Natalia Rivera3, Eva Galindez-Agirregoikoa1, Eduardo Cuende4, Ana Rosa Intxaurbe5, Juan M Blanco Madrigal1, Lucia Vega-Alvarez1, Carmen Lucia Garcia-Gomez6, Maria Enjuanes-Noguero7, Olaia Fernandez-Berrizbeitia8, Maria Rosa Exposito Molinero9, Maria Esther Ruiz Lucea1, Ignacio Torre Salaberri5 and iñigo Gorostiza Hormaeche1, 1Basurto University Hospital, Bilbao, Spain, 2Hospital universitario de Basurto, Bilbo, Spain, 3Biocruces Bizkaia Health Research Institute, Research area, Bilbao, Spain, 4Basurto University Hospital, Rheumatology, Madrid, Spain, 5Basurto University Hospital, Rheumatology, Bilbao, Spain, 6Basurto University Hospital, Rheumatology, Terrassa, Spain, 7Hospital Universitario de Basurto, Bilbao, Spain, 8Spanish Health Care Service, Bilbao, Spain, 9Hospital de Basurto, Bilbao, Spain
Background/Purpose: Before COVID pandemic, rheumatologists were not confident with telehealth for the need to adquire new technology, need of specific training and poorer reimbursement (1). Two groups of rheumatoid arthritis (RA) patients have been identified in a study of PROMS-based telehealth use (2): the keen and the reluctant.
Explore the degree of acceptance of asynchronous telehealth followup with whatsapp platform chatbot among our controlled AxSPA patients under biological therapy, and to search for a patient profile more prone to telehealth consultation
Methods: A prospective study with retrospective control was performed, choosing AxSPA patients under biological therapy with stable disease, visited in our center from 01/01 to 30/11/2021. We recruited 62 patients, but finally include 60 (2 quit for personal reasons). We offered them two teleconsultation visits (using their personal mobile), every f4 months, and a presential final visit one year after inclusion. The chatbot sends PROMS (BASDAI, VAS for patient global disease assessment, ASDAS, and 3 questions for extraarticular disease), and feedback and schedule for the following visits. In the case of lab test or PROMs deviation or when the patient asks for contact, it is phoned by nurse/doctor who solves the question and/or arranges an additional presential visit. We collect patient and disease characteristics (age, gender, educational level, employment, disease activity, duration and treatments), and patient ́s satisfaction and preferences in the final visit.
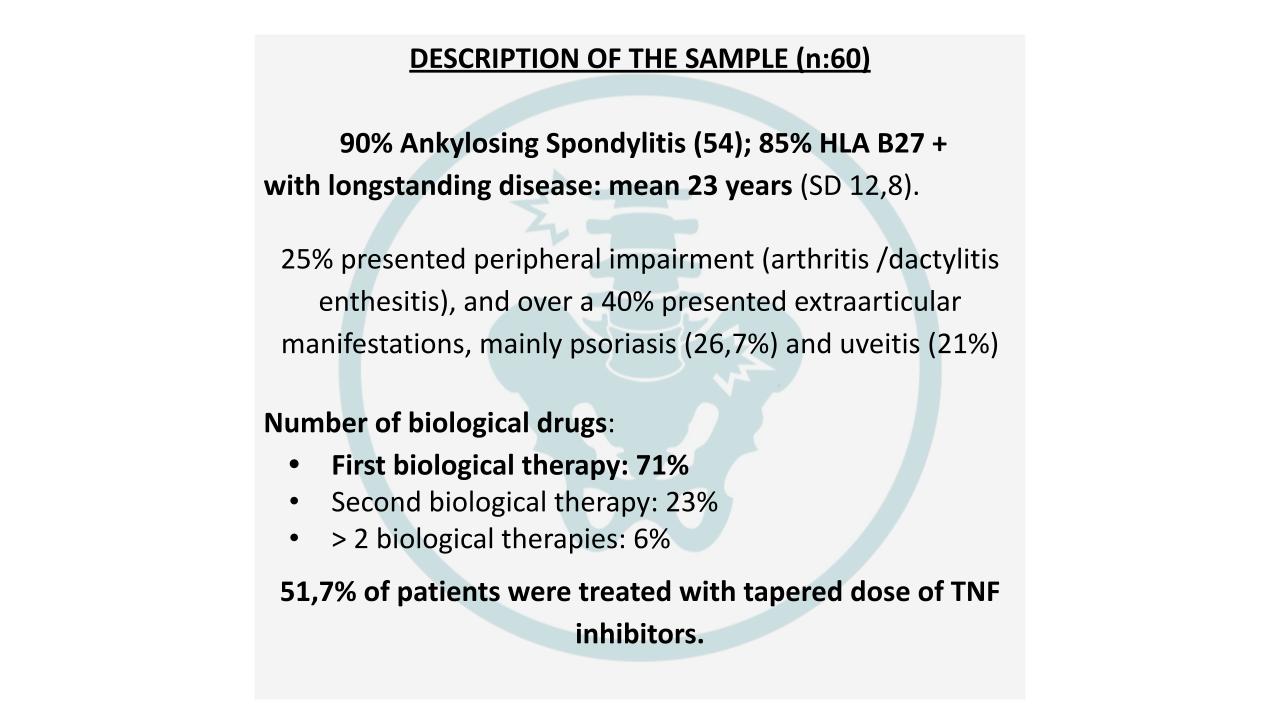
Results: We included 60 patients (Image 1).
At inclusion 93,3% were at remission/LDA by ASDAS/BASDAI-RCP and 4 patients were considered clinically controlled in spite of higher scores. At follow-up 3 patients with reduced dose needed to increase to standard dose of biological drug. There was no worsening from basal to final visits according BASDAI, BASFI, ASDAS-RCP or AsQOL.
Patients final VAS score (1-10) assessment of telehealth consultation was high: mean 9,14 ( DS 1,498); 91.7% ≥ 8 and 76.7% ≥ 9.
83,3% preferred telehealth follow-up. There was a trend towards telehealth preferences in higher educational levels, and active working (86% vs 70%) but not statistically significant. We found no correlation with gender, age and disease characteristics tested.
Conclusion: Asynchronous teleconsultation seems promising, not inferior to presential consultation and preferred for follow-up by our AxSpa patients with stable disease with biological drugs . We met some “reluctant patients”, that were more inactive working and with lower educational levels, but the differences were not significant. Further reserarch is needed with this telehealth model in other age and disease populations (RA), in order to characterize the reluctant and keen patients.
References: Muehlensiepen F, et al. Acceptance of Telerheumatology by Rheumatologists and General Practitioners in Germany: Nationwide Cross-sectional Survey Study. J Med Internet Res. 2021 Mar 29;23(3):e23742.
Knudsen LR, et al. Experiences With Telehealth Followup in Patients With Rheumatoid Arthritis: A Qualitative Interview Study. Arthritis Care Res (Hoboken). 2018 Sep;70(9):1366-1372.
Image 1
M. Garcia Vivar: None; e. abad plou: None; N. Rivera: None; E. Galindez-Agirregoikoa: None; E. Cuende: None; A. Intxaurbe: None; J. Blanco Madrigal: None; L. Vega-Alvarez: None; C. Garcia-Gomez: None; M. Enjuanes-Noguero: None; O. Fernandez-Berrizbeitia: None; M. Exposito Molinero: None; M. Ruiz Lucea: None; I. Torre Salaberri: None; i. Gorostiza Hormaeche: None.