Session: (0993–1012) Health Services Research Poster II
1001: Distance Not Travelled in a Tele-Rheumatology Shared Care Model: Leveraging the Expertise of an Advanced Clinician Practitioner in Arthritis Care (ACPAC)-trained Extended Role Practitioner (ERP) in Rural-remote Ontario
Amanda Steiman1, Jocelyne Murdoch2, Rachel Shupak3, Taucha Inrig4 and Katie Lundon5, 1Sinai Health System, Toronto, ON, Canada, 2Arthritis Society, Toronto, ON, Canada, 3St. Michael's Hospital/University of Toronto, Toronto, ON, Canada, 4St. Michael's Hospital, Toronto, ON, Canada, 5University of Toronto, Toronto, ON, Canada
Background/Purpose: A shortage of Rheumatologists has led to gaps in inflammatory arthritis (IA) care in Canada. Amplified in rural-remote communities, the number of Rheumatologists practicing rurally cannot be meaningfully increased. Alternate care strategies must be adopted. The economic impact of a shared-care Telerheumatology model, utilizing a community-embedded Advanced Clinician Practitioner in Arthritis Care (ACPAC)-ERP and an urban-based Rheumatologist, is described in terms of the estimated travel cost-savings (distance not traveled) for both patients and the healthcare system.
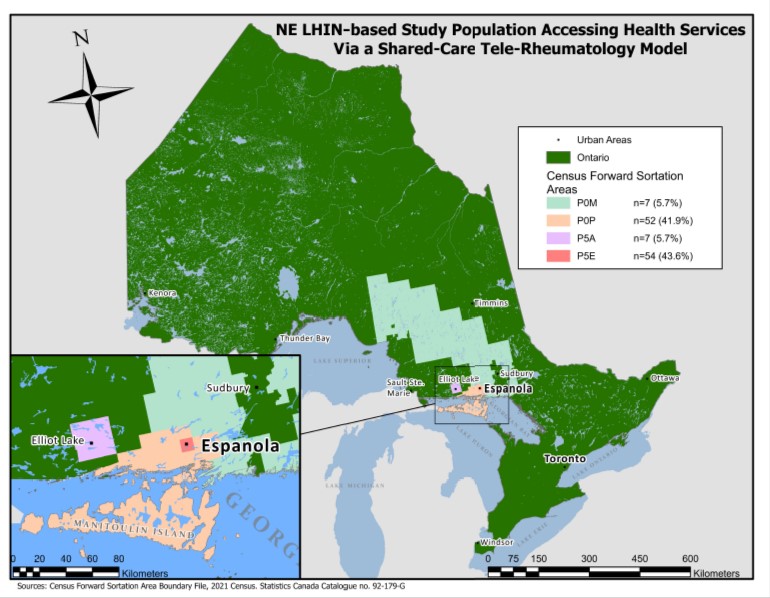
Results: Data from 124 patients seen between January 2013-January 2022 were collected: 98.0% (n=496/504 visits) were virtual. An estimated 493,470 km of patient-related travel was avoided (basedon 494 Telerheumatology visits). The loci where more than 5 patients resided is represented in Figure 1.A theoretical estimate of the MOH travel grant cost was $276,428, calculated based on the total number of patient visits that would have been incurred should these patients have been followed by the Rheumatologist in-person.
Conclusion: Half of a million kilometers (493,470 km) of travel was avoided for the patients involved in this Telerheumatology study, significantly reducing the carbon footprint and environmental impact by not travelling to access specialist rheumatology care. The estimated $276,428 cost-savings in this study represents a minimal base fiscal value of the ACPAC-trained ERP working within a Telerheumatology model of care. Other indirect costs need to be further captured in a more robust economic analysis. There is a compelling fiscal argument to support scaling-upof this model to deliver comprehensive and cost-effective virtual rheumatologic care in underserved communities provincially and beyond.
Figure 1.
A. Steiman: AstraZeneca, 1, GlaxoSmithKlein(GSK), 6, Pfizer, 5; J. Murdoch: None; R. Shupak: None; T. Inrig: Pfizer, 12, I was hired by Unity Health as a Research Coordinator, my salary was supported by a Pfizer unrestricted investigator-initiated grant; K. Lundon: None.