University Medical Center Ljubljana LJUBLJANA, Slovenia
Disclosure information not submitted.
Alojzija Hocevar1, JAKA OSTROVRŠNIK2, vESNA JURČIĆ3, Matija Tomšič4 and Ziga Rotar5, 1Department of Rheumatology, Universitiy Medical Centre Ljubljana, Ljubljana, Slovenia, 2UKC Ljubljana, Ljubljana, Slovenia, 3University of Ljubljana, Medical Faculty, Institute of Pathology, Ljubljana, Slovenia, 4Department of Rheumatology, University Medical Centre LJubljana, Ljubljana, Slovenia, 5University Medical Centre Ljubljana, Ljubljana, Slovenia
Background/Purpose: Data on survival of adults with IgA vasculitis (IgAV) are scarce. The aim of our study was to estimate for the first time the survival of IgAV patients in our country.
Methods: Our cohort consisted of adult patients diagnosed with IgAV between January 2010 and July 2022 and followed at our secondary/tertiary rheumatology center. To study the survival/mortality the censor date of 22, December 2022 was set, and time until death or the censor date, whichever came first, was recorded. Kaplan–Meier analysis and standardized mortality ratio (SMR) were plotted using survival data from age and sex matched Slovenian population as a reference. Cox proportional hazards regression analysis was used to study prognostic factors for mortality in IgAV.
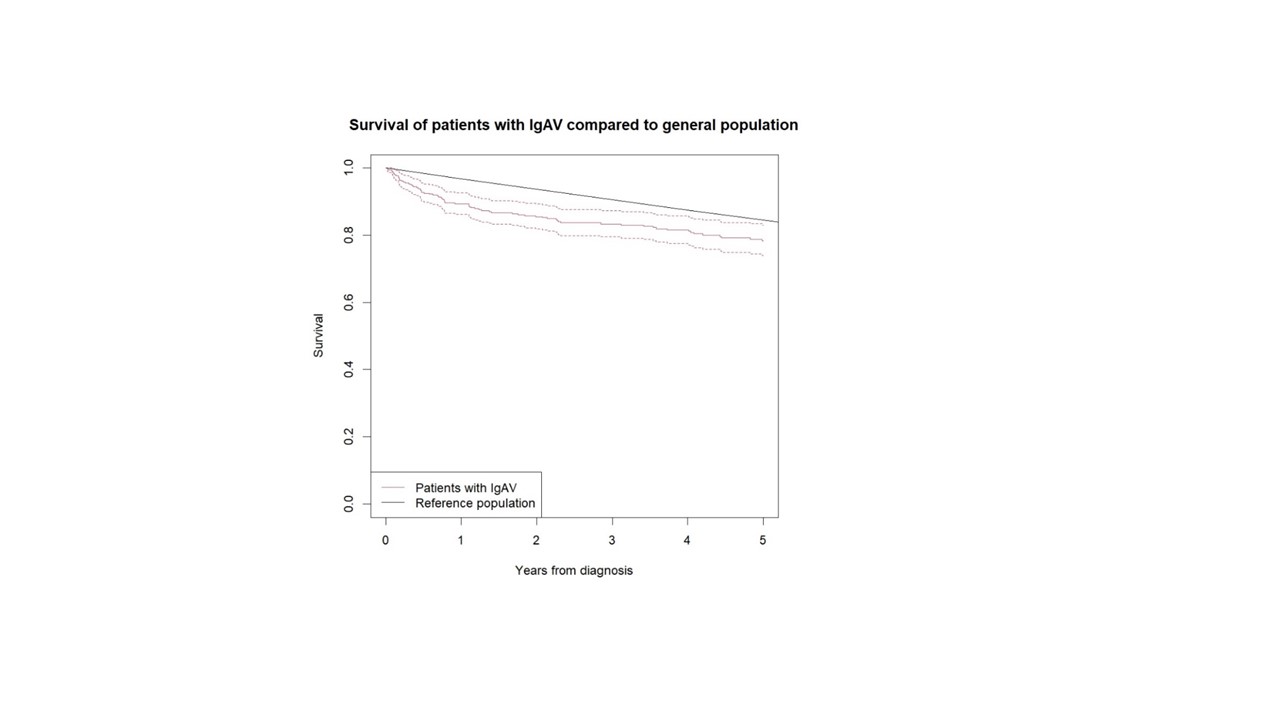
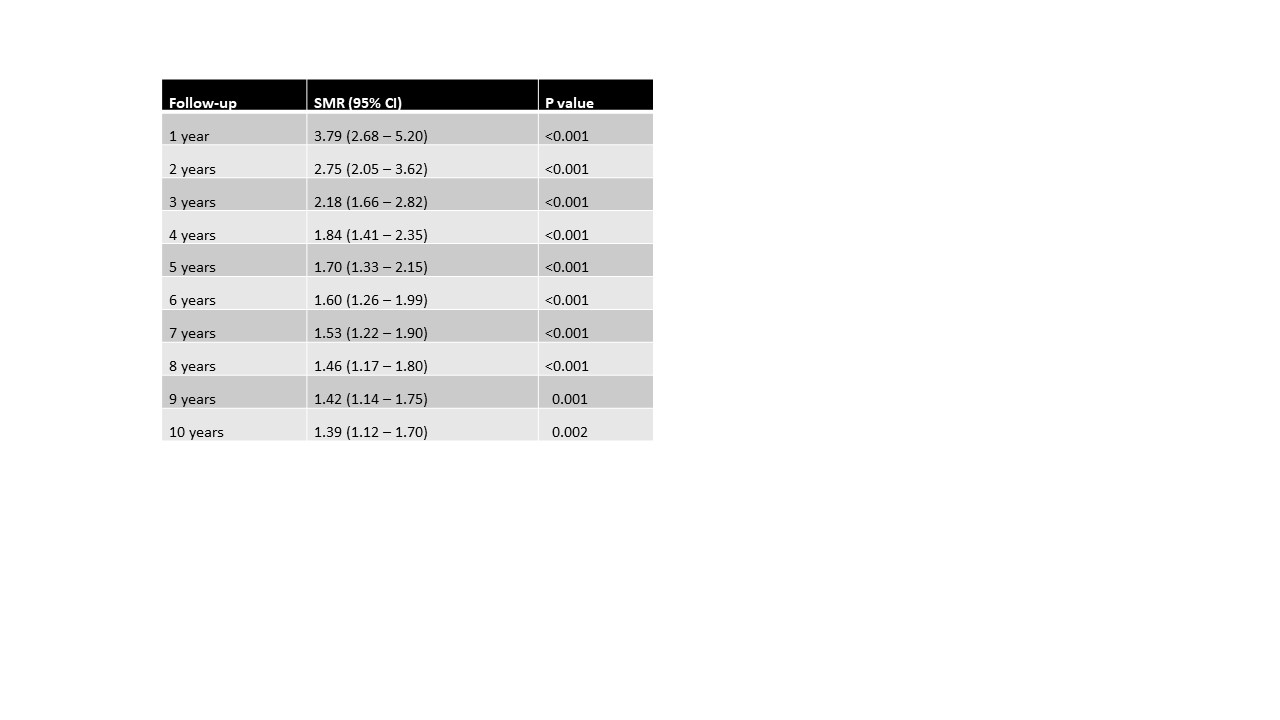
Results: Of 265 IgAV patients (156 (58.9%) males, median (IQR) age at diagnosis 61 (44; 74) years; median (IQR) follow up time 62 (27; 93) months), 48 (18.1%) patients died. Five-year survival in our cohort was 78% (95% CI 74%; 83%); in adults < 51 years 100% survival, and in adults aged ≥51 years 68% survival (the difference was significant, p=0.01). Ten-year survival in our patients was 65% (95%CI 59%; 72%). We found no sex related differences in the survival (p=0.37). The comparison of mortality between the IgAV cohort and age and sex matched general Slovenian population showed a significantly higher overall mortality in IgAV cohort, with an overall SMR of 1.4 (95%CI 1.14-1.71). The Kaplan-Meier survival curves of IgAV patients and matched general population as a comparator are shown in Figure 1. Excess deaths occurred mainly during the first two years of follow-up (Table 1). As risk factors associated with increased mortality in IgAV emerged patient age (HR 1.09 (95%CI 1.06; 1.13)), purpura above waistline (HR 2.14 (95% CI 1.13; 4.06)) and pre-existent heart failure (HR 7.37 (95%CI 3.74; 14.54)).
Cardiovascular diseases, cancer and infections represented the most frequent causes of death in our patients, recorded in 16 (33.3%), 6 (12.5%) and 6 (12.5%) patients, respectively, followed by hepatobiliary disease (3 cases), respiratory failure (2 cases), trauma/bleeding (3 cases) and dementia (3 cases). In one patient death was related to IgAV relapse, and in 8 (16.7%) patients the cause of death was unknown.
Conclusion: Survival of adults with IgAV was worse compared to matched general population in our country. Nevetheless, IgAV per se was an infrequent cause of death during follow up in our population.
Figure 1. Survival curve of IgAV patients according to Kaplan–Meier analysis compared to sex and age matched general Slovenian population
Table 1. The standardized mortality ratio of adults with IgAV . Legend: SMR standardized mortality ratio
A. Hocevar: None; J. OSTROVRŠNIK: None; v. JURČIĆ: None; M. Tomšič: None; Z. Rotar: None.