Irene Carrión-Barberà1, Laura Triginer2, Laura Tío2, Anna Pros3, Laia Belarte Tornero1, Sara Valdivielso More1, Sonia Ruiz Bustillo1, Joan Vime Jubany1, Nuria Farré López1 and Ronald Morales Murillo1, 1Hospital del Mar, Barcelona, Spain, 2Hospital del Mar Medical Research Institute (IMIM), Barcelona, Spain, 3Department of Rheumatology, Hospital del Mar, Barcelona, Spain
Background/Purpose: Systemic sclerosis (SSc) is a rare autoimmune connective tissue disease that can affect multiple organs including the heart. Primary heart involvement in SSc refers to the presence of cardiac fibrosis, inflammation, and dysfunction in the absence of pulmonary hypertension (PH). Although PH is usually considered one of the major risk factors for death in SSc patients, diastolic dysfunction (DD) has been proposed as an independent predictor of mortality, which may be more robust than PH. Early identification and management of heart complications in SSc patients are crucial to prevent further deterioration and improve treatment outcomes. However, myocardial damage caused by SSc is often poorly understood, and the long-term effects and prognosis remain unknown.
Our purpose is to study the prevalence and factors associated with left ventricular DD (LVDD) in a cohort of patients with SSc.
Methods: Cross-sectional study of 75 patients with SSc evaluated between Feb/2022 and Feb/2023. We classified patients as having LVDD as recommended by the 2016 American Society of Echocardiography/European Association of Cardiovascular Imaging (ASE/EACVI) guidelines. We compared the presence of factors associated with LVDD by performing first a bivariate analysis and lately a logistic regression adjusting by confounders (age, arterial hypertension (AH) and body mass index (BMI)).
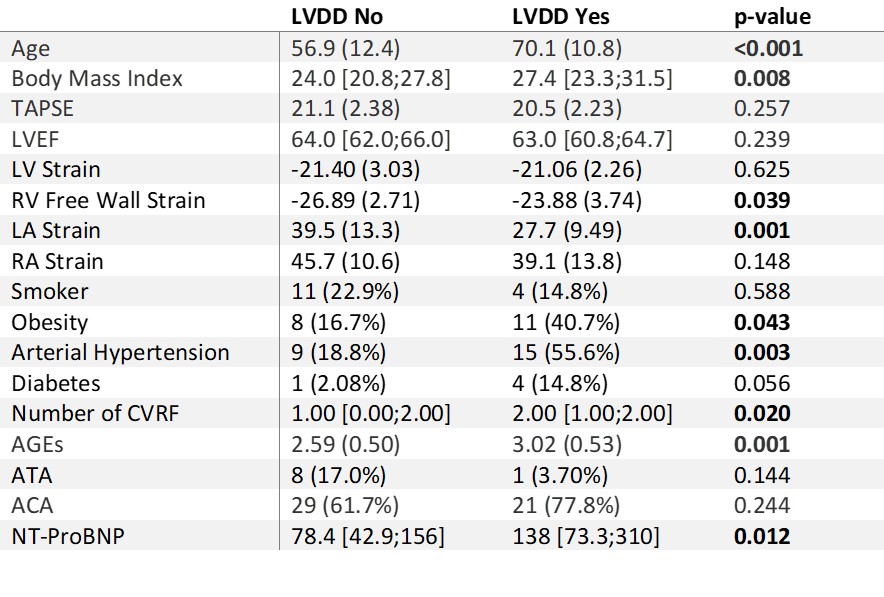
Results: Of the 75 patients, 27 (36%) had LVDD and 48 (64%) had normal diastolic function. Table 1 shows compared characteristics of both groups. Older age, AH, BMI, the total number of cardiovascular risk factors (CVRF), advanced glycation end products (AGEs), NT-proBNP levels, impairment of the right ventricular (RV) free wall strain, and lower left atrial (LA) strain reservoir function were significantly associated with having LVDD (Table 1), while classical parameters of ventricular function, such as left ventricular ejection fraction or tricuspid annular plane systolic excursion were not. After adjusting for confounding factors in the logistic regression, the presence of anticentromere antibodies (ACA) conferred a risk 32 times higher (OR 32.15 95%CI [1.3;775.86], p=0.03) for presenting LVDD than having anti-topoisomerase antibodies. An increase in 1 unit of AGEs also augmented the risk of LVDD almost 5 times (OR 4.9 95%CI [1.3;18.43], p=0.018).
Conclusion: LVDD is highly prevalent in SSc, particularly in elderly patients with a higher BMI, AH and more CVRF. LVDD is associated with higher levels of NT-proBNP and findings in less classical echocardiographic parameters like the RV free wall strain impairment and lower LA strain function. ACA and higher level of AGEs were associated with a significant increased risk of LVDD after adjusting for confounders. These findings highlight the importance of regular cardiovascular monitoring in SSc patients and the potential value of using new echocardiographic parameters to identify those at risk for LVDD.
Table 1: Difference in variables between patients with left ventricle diastolic dysfunction and not. Bold indicates p-value<0.05. LVDD: left ventricle diastolic dysfunction; TAPSE: tricuspid annular plane systolic excursion, LVEF: left ventricle ejection fraction; RV: right ventricle; LA: left atrium; RA: right atrium; CVRF: cardiovascular risk factors; AGEs: advanced glycation end products; ATA: anti-topoisomerase antibodies; ACA: anticentromere antibodies; NT-proBNP: aminoterminal pro B-type natriuretic peptide.
I. Carrión-Barberà: None; L. Triginer: None; L. Tío: None; A. Pros: None; L. Belarte Tornero: None; S. Valdivielso More: None; S. Ruiz Bustillo: None; J. Vime Jubany: None; N. Farré López: None; R. Morales Murillo: None.