National Psoriasis Foundation Alexandria, VA, United States
Disclosure information not submitted.
Lourdes Perez-Chada1, George Gondo2, Joseph F. Merola3 and Alice B. Gottlieb4, 1Brigham and Women's Hospital, Boston, MA, 2National Psoriasis Foundation, Alexandria, VA, 3Brigham and Women's Hospital and Harvard Medical School, Boston, MA, 4Icahn School of Medicine at Mount Sinai, New York, NY
Background/Purpose: The IDEOM MSK-Q aims to assess MSK symptoms in individuals with psoriatic disease. It consists of 3 subscales: Intensity of MSK Symptom (3 items), Impact of MSK Symptoms (4 items), and Intensity of Fatigue (1 item). This study sought to evaluate the known-groups validity of the IDEOM MSK-Q.
Methods: Data from a cross-sectional survey of a random sample of individuals with psoriasis was used. To determine the known-groups validity of the IDEOM MSK-Q, we compared the IDEOM MSK-Q score among different groups based on: A). Disease status: patients with psoriasis-only vs psoriasis with PEST ≥ 3 vs PsA; B). PEST score: PEST < 3 vs PEST ≥ 3; and C.) Impact of PsA: Psoriatic Arthritis Impact of Disease (PsAID-9) < 4 vs PsAID ≥ 4. ANOVA and ANCOVA, adjusting for age and sex, were used.
Results: A total of 1,453 participants completed the survey. Equal proportions of participants reported a physician given diagnosis of psoriasis-only (47.9%) and psoriasis with concomitant PsA (47.7%), and 4.4% only having PsA. Participants were mostly female (58.4%) with mild psoriasis (52.3% - BSA 3%). Mean participant age was 54.8 (SD ± 15.73). Among all participants, 61% had a PEST score ≥ 3, indicating the potential presence of PsA. Among individuals with PsA and those with psoriasis-only with a PEST score ≥ 3, 65.5% had a PsAID score > 4 (i.e., unacceptable symptom state). For all participants, mean scores for the for the Intensity of MSK Symptom, Impact of MSK Symptoms, and Fatigue subscales were 18.4 (SD = ± 13.9), 5.0 (SD = ± 3.3), and 5.01 (SD = ± 3.28).
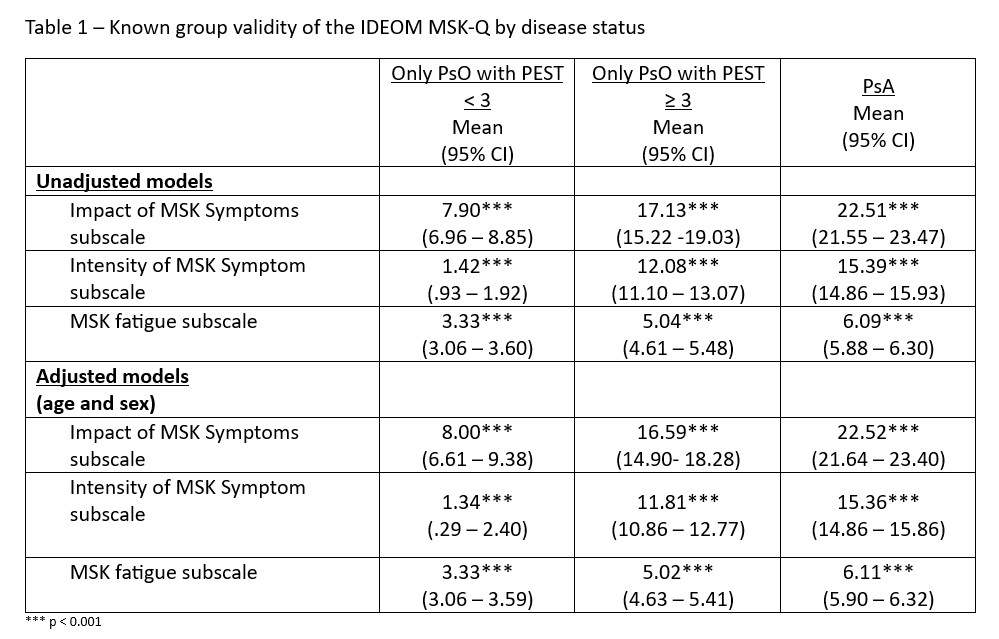
Results comparing the IDEOM MSK-Q subscales among different disease statues groups were statistically significant. Across all subscales, individuals with PsA scored higher than individuals with psoriasis with PEST score ≥ 3, and those with psoriasis-only (Table 1). These differences were maintained when adjusting for age and sex (see Table 1.)
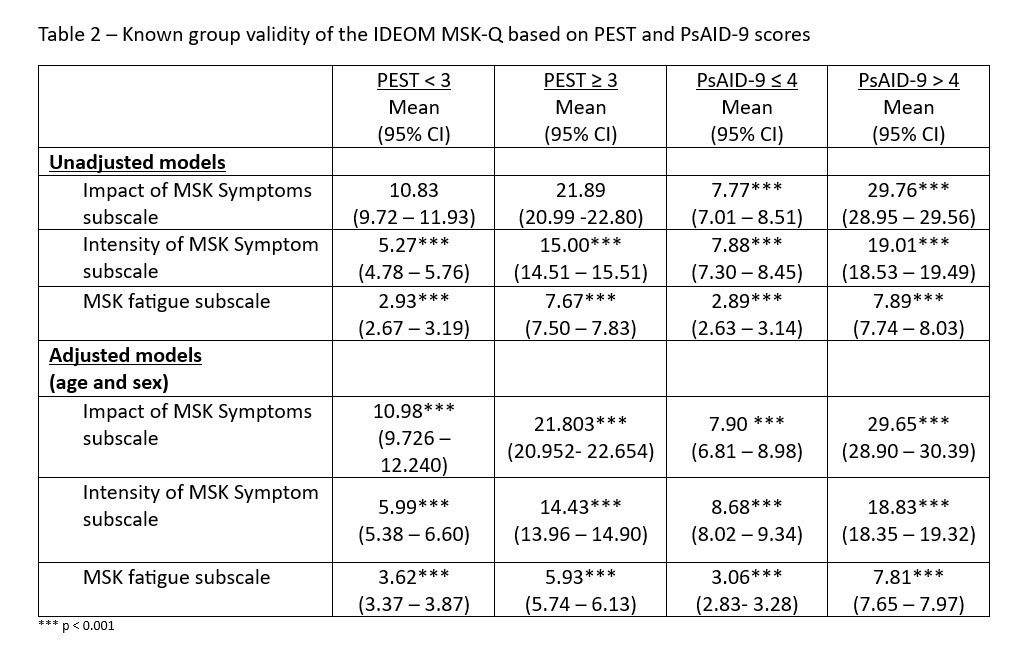
Unadjusted between group comparison based on PEST score (PEST < 3 vs PEST ≥ 3) were statistically significant for the Intensity of MSK Symptom and Impact of MSK Symptoms subscales. Participants who had a PEST > 3 scored higher across all components of the IDEOM MSK-Q (Table 2) compared to PEST < 3. Similarly, unadjusted group comparison based on PsAID score (PsAID ≤ 4 vs PsAID > 4) suggest that individuals at unacceptable symptom state (PSAID > 4) scored higher on all 3 subscales (Intensity of MSK Symptom, Impact of MSK Symptoms , and Fatigue) (Table2). After adjusting for age and sex, comparisons remained statistically significant (see Table 2).
Conclusion: Results from this study suggest that the IDEOM MSK-Q can discriminate between individuals based on disease status, PEST score, and impact of psoriatic arthritis reflecting it has good known group validity.
Table 1 – Known group validity of the IDEOM MSK-Q by disease status.
Table 2 – Known group validity of the IDEOM MSK-Q based on PEST and PsAID-9 scores.