Abstract Session
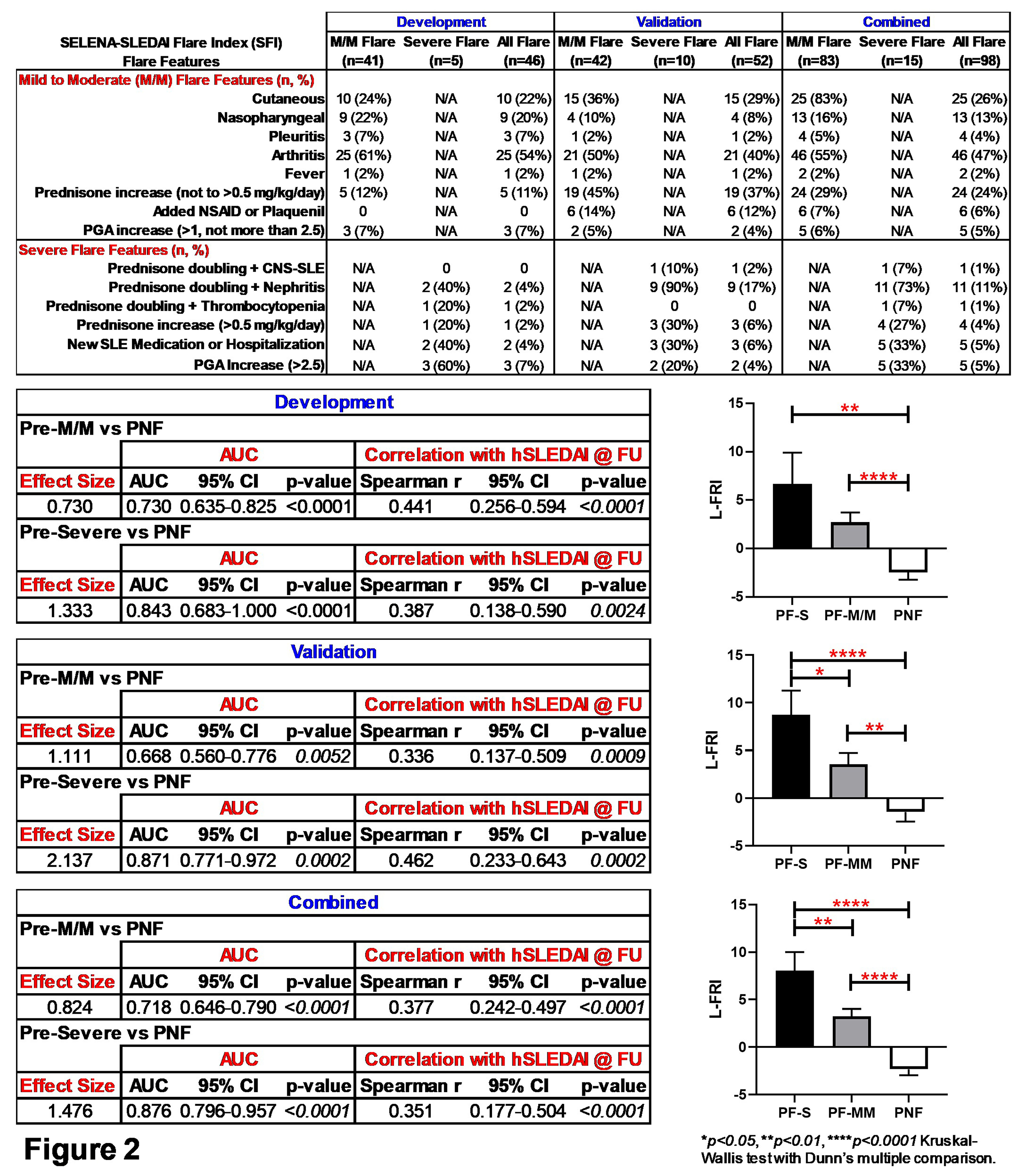
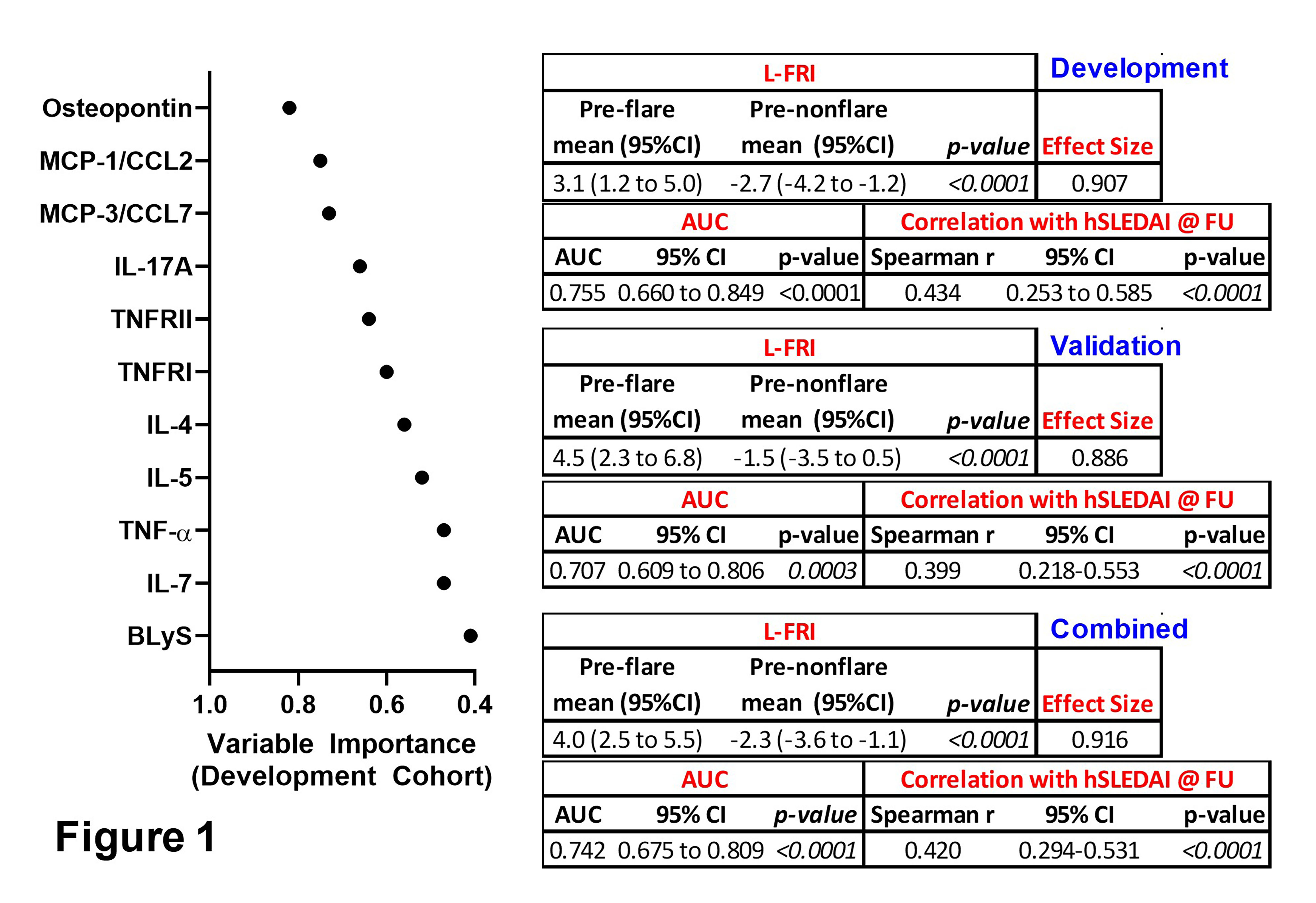
Systemic lupus erythematosus (SLE)


.png "Melissa Munroe, MD, PhD (she/her/hers) photo")
Melissa Munroe, MD, PhD (she/her/hers)
Oklahoma Medical Research Foundation
Oklahoma City, OK, United States
Disclosure information not submitted.
.jpg)