Brigham and Women's Hospital Hanover, NH, United States
Disclosure information not submitted.
Lindsey MacFarlane1, Hanna Mass1, Catherine Yang1, Jose Acosta Julbe1, Antonia Chen1, Jeffrey Lange1, Morgan Jones1, Faith Selzer1, Jamie Collins1, Elena Losina2 and Jeffrey Katz1, 1Brigham and Women's Hospital, Boston, MA, 2Brigham and Women's Hospital, Boston, MA
Background/Purpose: Pain in knee osteoarthritis (OA) is multifactorial and influenced by factors including pain sensitization. Most literature on sensitization and OA has contrasted persons with and without OA. We examined the association between knee pain severity and sensitization in a cohort of persons with OA. Further, within individuals with discordant knee pain, we compared sensitization between knees.
Methods: We recruited patients with knee OA from an orthopedic practice. Knee pain was assessed in each knee using the Knee Injury and Osteoarthritis Outcome Score (KOOS 0-100, 100 best) and categorized into tertiles; higher (< 47 points), moderate (³47 points and < 69), and lower (³ 69 points). We considered individuals to have 'discordant pain' if one knee was in the highest tertile and the other in the lowest. Participants underwent quantitative sensory testing (QST) including pain pressure threshold (PPT), temporal summation (TS), and conditioned pain modulation (CPM). We measured PPT at each knee and one wrist. We assessed TS at each knee and 3rd digit. We calculated CPM efficiency as the ratio of mean PPT testing at the wrist before and after the conditioning stimulus (PPT post/PPT pre). Higher TS scores and lower PPT and CPM indicate greater sensitization. We assessed PPT and TS at the knee in knee level analyses and CPM, PPT at the wrist and TS at the digit in person level analyses.
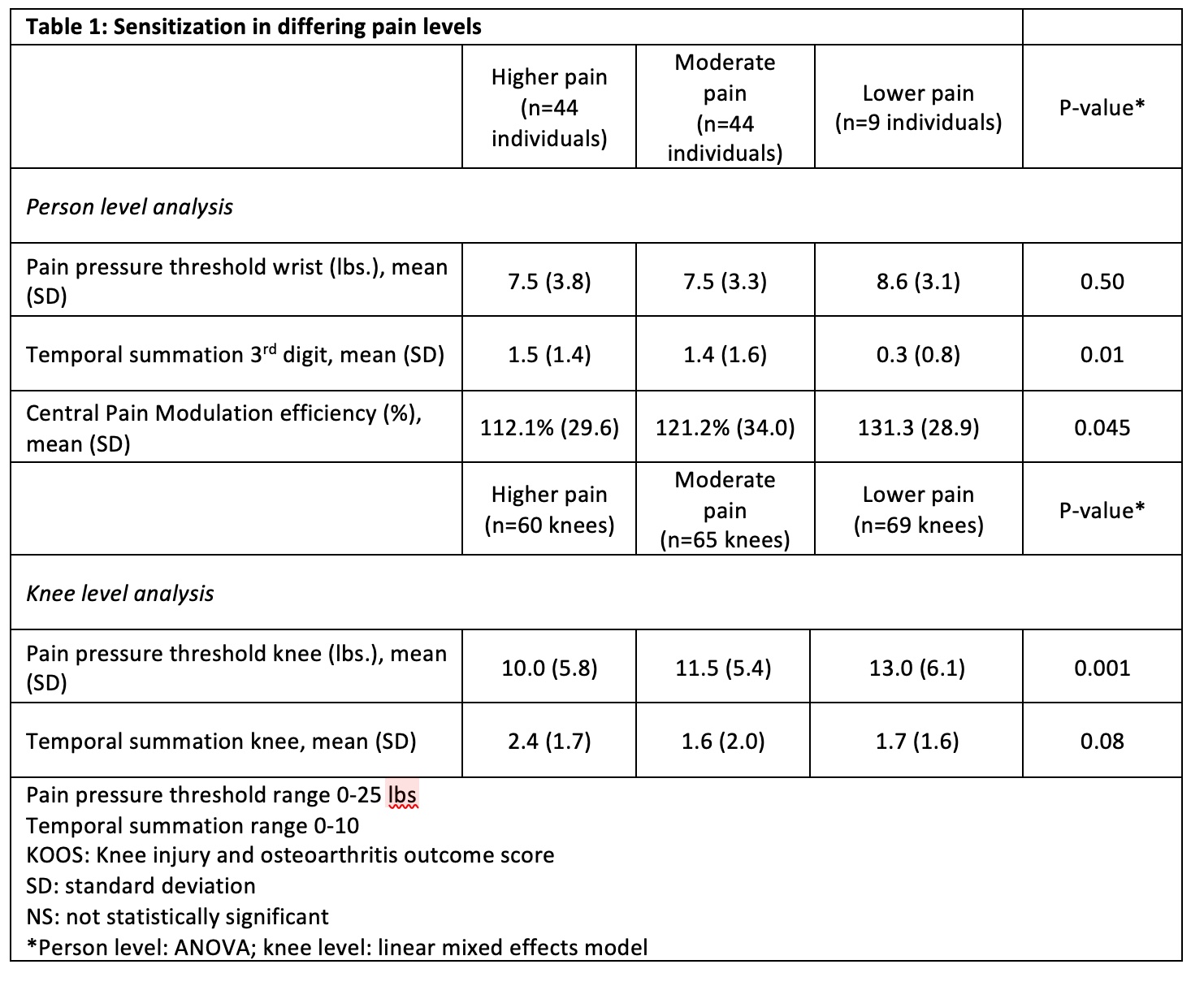
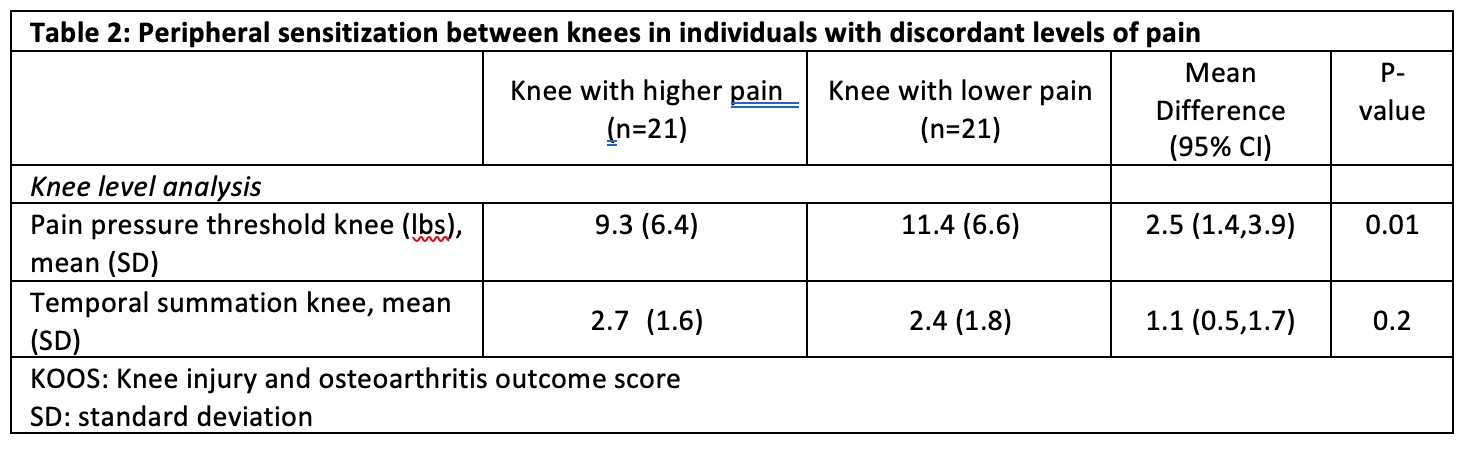
We investigated the relationship between knee pain and sensitization in knee-level and person-level analyses. In person level analyses, we classified individuals into pain tertiles of their most painful knee and examined differences across persons in CPM efficiency, TM at the 3rd digit, and PPT of the wrist. We assessed differences in sensitization between knee pain tertiles using ANOVA. In knee level analyses, we used linear mixed effect models to account for within person correlations. We used paired t-tests to compare differences in QST between discordant knees within an individual.
Results: The sample included 194 knees from 97 participants. Participants had a mean age of 64 years (SD 11), BMI of 30 (SD 8), and 63 (72%) were female. In person level analyses, we observed differences in TS at the 3rd digit across the pain severity tertiles with TS of 1.5 (SD 1.4) in the higher pain group vs 0.3 (SD 0.8) in the lower. We observed small (< 0.5 SD) person level differences across pain tertiles in PPT of the wrist and CPM (Table). In knee level analyses, we observed PPT at the knee increased modestly across pain tertiles. Among the 21 individuals with discordant knee pain, the more painful knee demonstrated modestly lower PPT at the knee (differences < 0.5 SD).
Conclusion: These data support prior research demonstrating greater sensitization in persons with greater knee pain. Our design permitted investigation of sensitization at the knee level. While knees with more pain (across persons and within person), generally had greater sensitization than knees with less pain, the magnitude of these differences was small. The limited influence of sensitization on knee pain in these cross-sectional analyses suggests investigators should have modest expectations of the efficacy of treatments targeting sensitization.
Sensitization in differing pain levels
Peripheral sensitization between knees in individuals with discordant levels of pain
L. MacFarlane: None; H. Mass: None; C. Yang: None; J. Acosta Julbe: None; A. Chen: Adaptive Phage Therapeutics, 2, 5, Avanos, 2, BICMD, 2, Convatec, 2, Elute, 5, Ethicon, 2, GLG, 2, Guidepoint, 2, Heraeus, 2, Hyalex, 11, IlluminOss, 11, IrriMax, 2, Osteal Therapeutics, 2, 11, Peptilogics, 2, 11, Pfizer, 2, Smith and Nephew, 2, Sonoran, 11, Stryker, 2, 9; J. Lange: Aesulap, 2, OnPoint Kneee, 4; M. Jones: Biosplice, 1, 2, Pacira, 5, Regeneron, 1, 2; F. Selzer: None; J. Collins: None; E. Losina: None; J. Katz: Biosplice, 5.