Chris Lane1, Louise Thoma2, Carolina Alvarez3, Deborah Givens4, Amanda Nelson4, Adam Goode5, Kharma Foucher6 and Yvonne Golightly7, 1UNC Chapel Hill, Chapel Hill, NC, 2University of North Carolina, Chapel Hill, NC, 3University of North Carolina at Chapel Hill, Miami, FL, 4University of North Carolina at Chapel Hill, Chapel Hill, NC, 5Duke University, Durham, NC, 6University of Illinois at Chicago, Chicago, IL, 7University of Nebraska Medical Center, Omaha, NE
Background/Purpose: Sex and race differences have been observed in clinical outcomes such as patient-reported pain and function in adults with knee OA. However, few studies have examined sex and race differences in vibration sensitivity and pressure pain sensitivity, which may better represent neurophysiological changes suggestive of longer-term symptoms. The purpose of the study was to examine if associations of these neurophysiological assessments with knee OA outcomes differ across sex and race, which may contribute to known sex and race disparities in clinical outcomes.
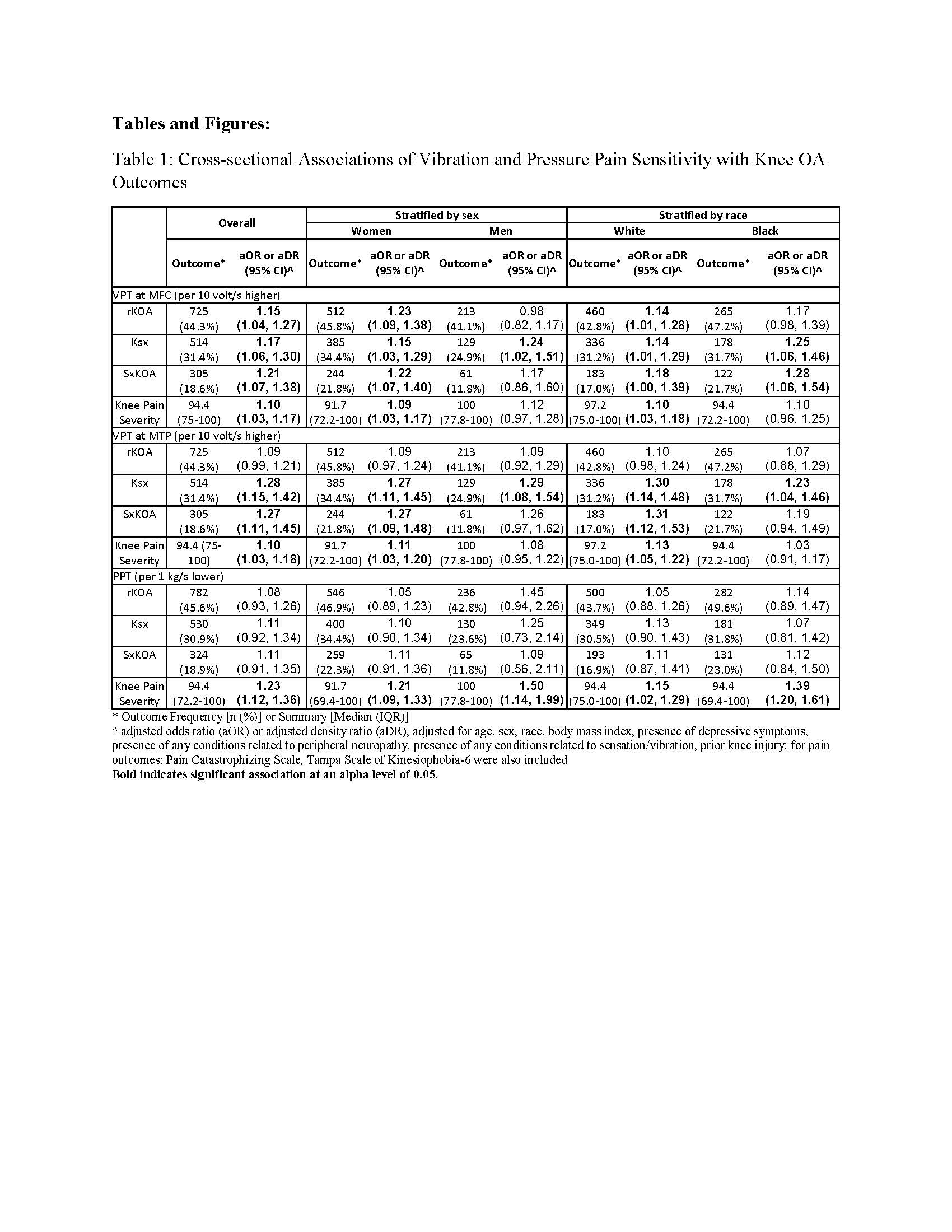
Methods: Data were from the 2013-2015 follow-up of the Johnston County Osteoarthritis Project. Exposures were vibration perception threshold (VPT) and pressure pain threshold (PPT). VPT was measured using a biothesiometer operating at 120 Hz at the bilateral medial femoral condyle (MFC) and first metatarsophalangeal joint (MTP). PPT was measured on a 0-4 kg scale using a standard mechanical pressure-based dolorimeter operating at 1 kg/sec at the bilateral upper trapezius. Outcomes were frequency of radiographic knee OA (rKOA, defined as Kellgren-Lawrence grade 2–4), Ksx (defined as knee pain, aching, or stiffness on most days of any one month in the last 12 months regardless of rKOA status), symptomatic knee OA (sxKOA, defined as having both rKOA and knee symptoms), and knee pain severity (measured with Knee Injury and Osteoarthritis Outcome Score (KOOS) Pain Subscale) in each knee. We examined cross-sectional associations of the exposures with the outcomes using separate logistic regression models to calculate odds ratios for dichotomous outcomes and log linear models to calculate density ratios for knee pain severity, with 95% confidence intervals. Limb-level models were assessed using generalized estimating equations to account for correlations between limbs and adjusted for relevant covariates (Table 1). Results were presented for the overall sample and separately by sex or race.
Results: Of 851 and 862 participants available for the VPT and PPT analysis (mean age 71 years, 2/3 female, 1/3 Black, BMI 31 kg/m2), 1585 and 1660 knees were used for complete case analysis, respectively. Higher VPT (higher threshold for vibration perception) at the MFC and MTP was associated with the presence of all outcomes. Lower PPT (lower threshold for pain) was associated with greater knee pain severity. Estimates of associations of VPT with all outcomes were similar among women and men but some estimates were less precise (wider confidence interval) among men than women. Estimates for PPT were similar among men and women. Estimates of associations of VPT and PPT with all outcomes were similar among White and Black adults but some estimates were less precise among Black adults than White adults (Table 1).
Conclusion: Diminished vibration perception and greater pressure pain sensitivity were cross-sectionally associated with worse knee OA outcomes. Associations were similar across sex and race groups, suggesting the neurophysiological assessments do not largely inform established sex and race disparities in clinical outcomes.
C. Lane: None; L. Thoma: None; C. Alvarez: None; D. Givens: None; A. Nelson: None; A. Goode: None; K. Foucher: None; Y. Golightly: None.