0286: Relationship Between High Resolution Computed Tomography(HRCT) Quantitative Scores and Physiological and Clinical Features in Antisynthetase Syndrome Related Interstitial Lung Disease
Sangmee Bae1, Fereidoun Abtin2, Grace Kim3, Daniela Markovic4, Siamak Moghadam-Kia5, Chester V. Oddis6, Lila Pourzand2, Didem Saygin6, Daniel Sullivan7, Koichi Yamaguchi5, Donald Tashkin3, Christina Charles-Schoeman8, Jonathan Goldin3 and Rohit Aggarwal6, 1UCLA Rheumatology, Los Angeles, CA, 2UCLA Radiological Sciences, Los Angeles, CA, 3University of California Los Angeles, Los Angeles, CA, 4UCLA Department of Medicine Statistics Core, Los Angeles, CA, 5University of Pittsburgh Medical Center Rheumatology, Pittsburgh, PA, 6University of Pittsburgh, Pittsburgh, PA, 7UCLA Pulmonology, Pittsburgh, PA, 8UCLA Medical Center, Santa Monica, CA
Background/Purpose: High resolution chest computed tomography (HRCT) plays an important role in the clinical evaluation of interstitial lung disease (ILD) by demonstrating the extent of parenchymal disease and detecting serial changes over time. A quantitative CT scoring method using a computer aided diagnosis system to measure the nature and extent of parenchymal diseases has been used to measure treatment response in the scleroderma lung study II (SLSII). The current study aims to evaluate the association of quantitative CT scores and clinical/physiological disease parameters in a cohort of antisynthetase positive myositis patients with ILD.
Methods: We analyzed 20 patients enrolled at the Abatacept in Myositis Associated Interstitial lung disease (Attack My-ILD) study. Myositis patients with antisynthetase antibodies and active ILD were enrolled across 5 centers and randomized to a double blind placebo period for 24 weeks followed by an open label period for 24 weeks. HRCT were performed at 3 timepoints (week 0, 24, 48) with quantitative scores for extent of ground glass (QGG), fibrosis (QLF), total ILD (QILD) performed using a computer aided diagnostic system. Pulmonary function tests (forced vital capacity [FVC], diffusing capacity adjusted for hemoglobin [DLCO]), 6 minute walk distance (6MWD), physician/patient reported outcomes (UCSD shortness of breath questionnaire, short form-36 (SF-36), Borg scale, myositis disease activity assessment tool (MDAAT), health assessment questionnaire (HAQ), patient global myositis activity visual analog scale, supplemental oxygen use) were all obtained over 5 timepoints (wk 0, 12, 24, 36, 48). Associations between quantitative CT scores with various physiologic and clinical parameters were analyzed using Spearman's correlations cross-sectionally at baseline, and mixed effect models were used to analyze associations longitudinally over multiple timepoints.
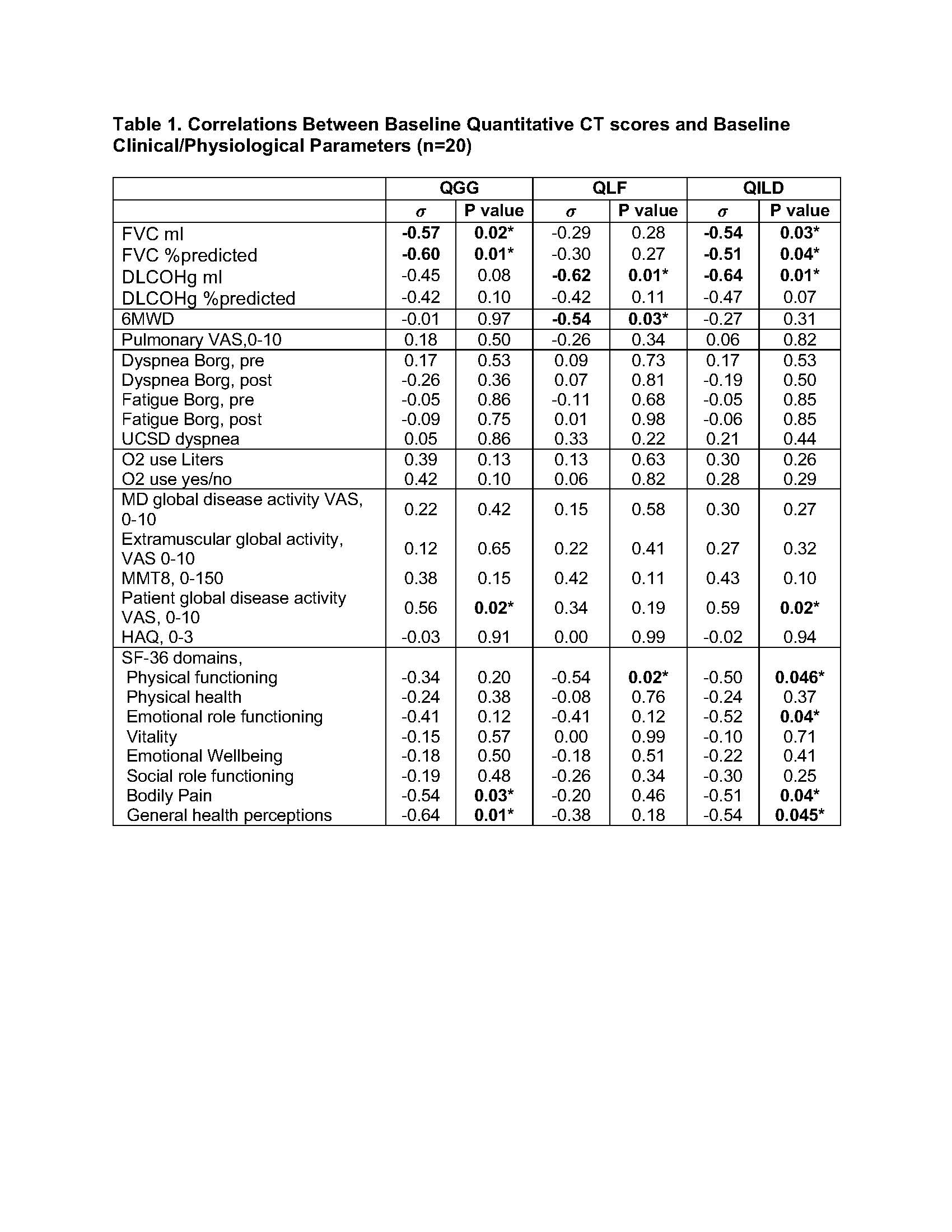
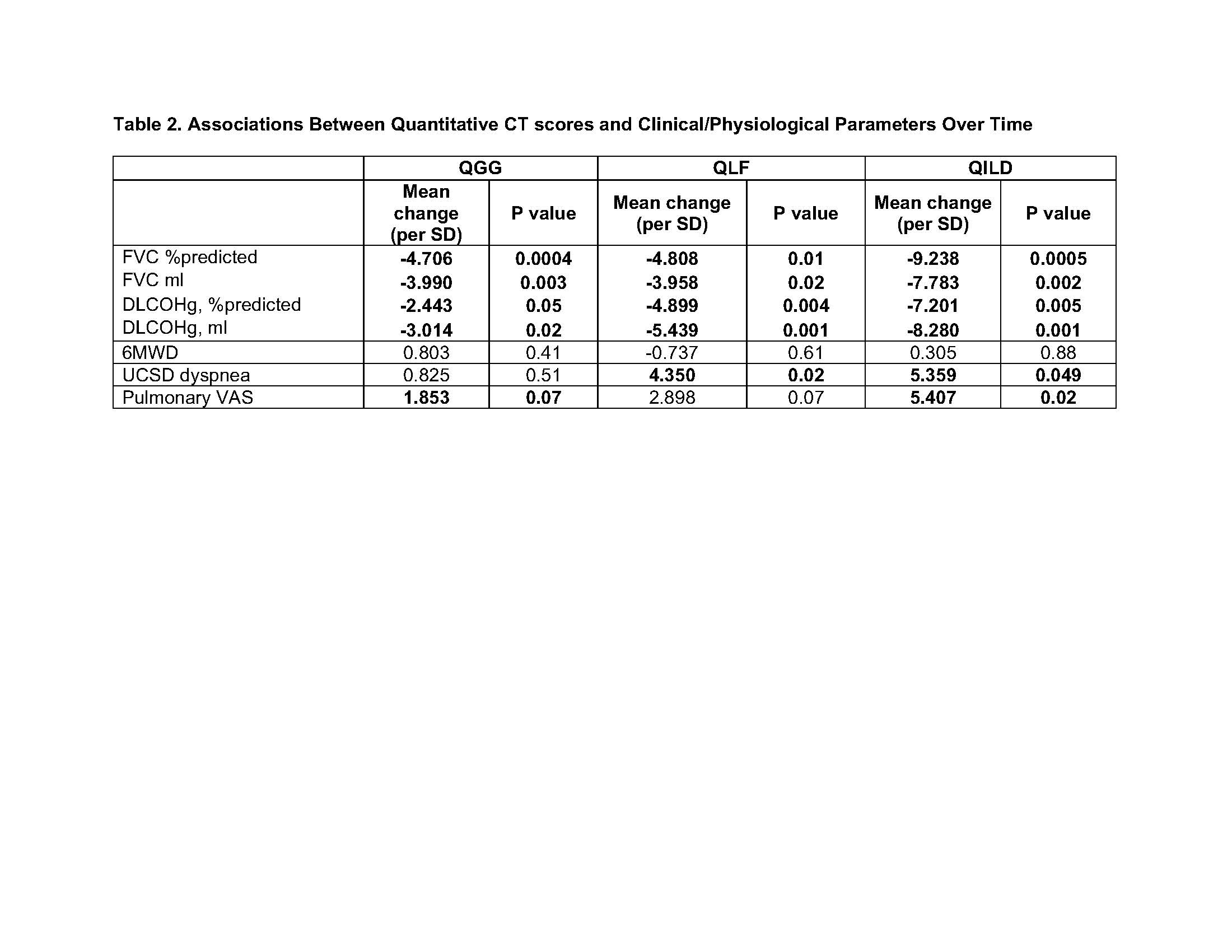
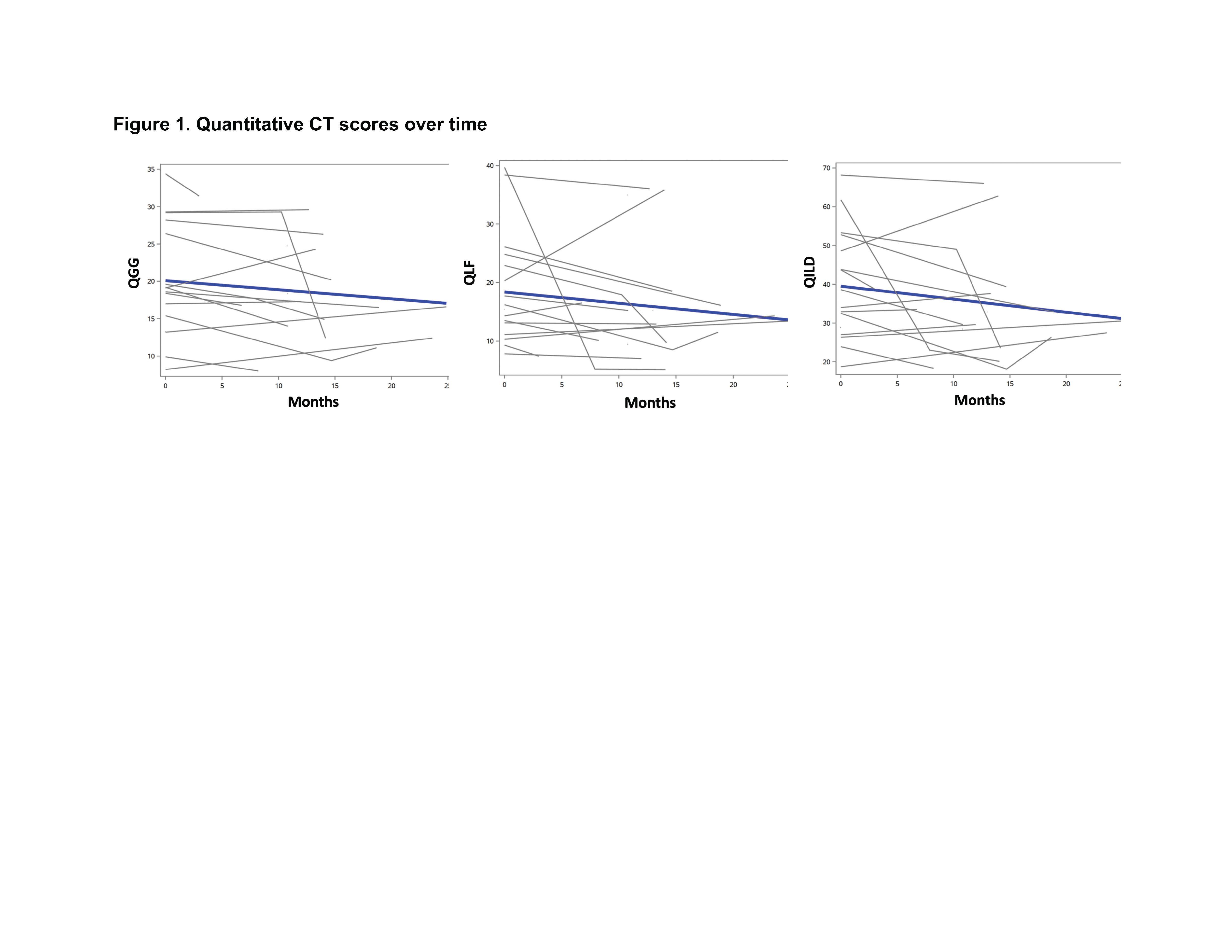
Results: Baseline quantitative CT scores for total extent of ILD (QILD) had strong inverse correlations with baseline FVC and DLCO, while ground glass (QGG) had strong inverse correlations with FVC and fibrosis(QLF) had strong inverse correlations with DLCO (Table 1). Baseline QGG and QILD also correlated with higher scores on patient reported global disease activity and worse health status on several SF-36 domains, whereas QLF correlated with shorter 6MWD and worse physical functioning (Table 1). Using mixed effect models, quantitative CT scores assessed over time demonstrated strong associations between all quantitative CT scores (QGG, QLF, QILD) and both FVC as well as DLCO (Table 2). QLF and QILD scores were also associated with worse scores of respiratory status reported by the patient and physician (UCSD shortness of breath questionnaire and pulmonary VAS on the MDAAT) but were not associated with the 6MWD. The estimated trajectories for quantitative CT scores over time trended towards improved CT scores overall (Figure 1).
Conclusion: Higher quantitative CT scores measuring the extent of ground glass (QGG), fibrosis(QLF), and total ILD (QILD) correlated with pulmonary function tests as well as patient and physician reported outcomes of respiratory status over time in patients with myositis related ILD.
σ Spearman’s Rho for correlation coefficient *p<0.05 Abbreviations: QILD, quantitative ILD score on HRCT; QGG, quantitative ground glass score on HRCT; QLF, quantitative fibrosis score on HRCT; FVC, forced vital capacity, DLCO Hg, diffusion capacity adjusted by hemoglobin, UCSD Dyspnea score, University of California San Diego Shortness of Breath Questionnaire with higher scores for worse dyspnea; Pulmonary VAS, pulmonary visual analog scale from the Myositis disease activity assessment tool (MDAAT); Borg scale, Borg scale for dyspnea and fatigue before and after test with higher score indicating more severe symptoms.
Values reported are mean change per standard deviation estimated using mixed effect models
Blue lines are estimated trajectories of CT scores (QGG, QLF, QILD) over time(months) using mixed effect models
S. Bae: None; F. Abtin: None; G. Kim: MedQIA, 2; D. Markovic: None; S. Moghadam-Kia: None; C. V. Oddis: Boehringer-Ingelheim, 5, Cabaletta, 5, EMD Serono, 5, Novartis, 5, Pfizer, 1; L. Pourzand: None; D. Saygin: None; D. Sullivan: None; K. Yamaguchi: None; D. Tashkin: None; C. Charles-Schoeman: AbbVie, 2, 5, Alexion, 5, BMS, 2, 5, Boehringer Ingleheim, 2, 5, CSL Behring, 5, Galapagos, 2, Pfizer, 2, 5, Priovant, 2, 5, Recludix, 2; J. Goldin: MedQIA, 12, Founder; R. Aggarwal: Actigraph, 2, Alexion, 2, ANI Pharmaceuticals, 2, Argenx, 2, AstraZeneca, 2, Boehringer-Ingelheim, 2, 5, Bristol-Myers Squibb(BMS), 2, 5, CabalettaBio, 2, Capella Bioscience, 2, Corbus, 2, CSL Behring, 2, EMD Serono, 2, 5, Galapagos, 2, Horizon Therapeutics, 2, I-Cell, 2, Janssen, 2, 5, Kezar, 2, Kyverna, 2, Mallinckrodt, 5, Merck, 2, Octapharma, 2, Pfizer, 2, 5, Q32, 5, Roivant, 2, Sanofi, 2, Teva, 2.