Courtney Hoge1, C. Barrett Bowling2, Charmayne Dunlop-Thomas1, Bradley Pearce1, S. Sam Lim1, Cristina Drenkard1 and Laura Plantinga1, 1Emory University, Atlanta, GA, 2Duke University, Durham, NC
Background/Purpose: Physical performance is often not measured in clinical settings, despite its association with increased risk of disability, loss of independence, and mortality. Here, we sought to examine the prevalence and correlates of poor physical performance among individuals with systemic lupus erythematosus (SLE) who were recruited from a primarily Black, population-based cohort in Atlanta.
Methods: Participants were recruited for an ancillary study from the ongoing, population-based Georgians Organized Against Lupus (GOAL) cohort of individuals with SLE. Those who had complete Short Physical Performance Battery [SPPB: score range, 0-12; intermediate-low (< 10) vs. high (≥10)] data from either an in-person or a remote study visit (10/8/19-5/12/22) were included. Demographic, clinical, and psychosocial variables were summarized, and the associations [adjusted odds ratios (aOR)] of intermediate-low vs. high physical performance with these characteristics were estimated via multivariable logistic regression.
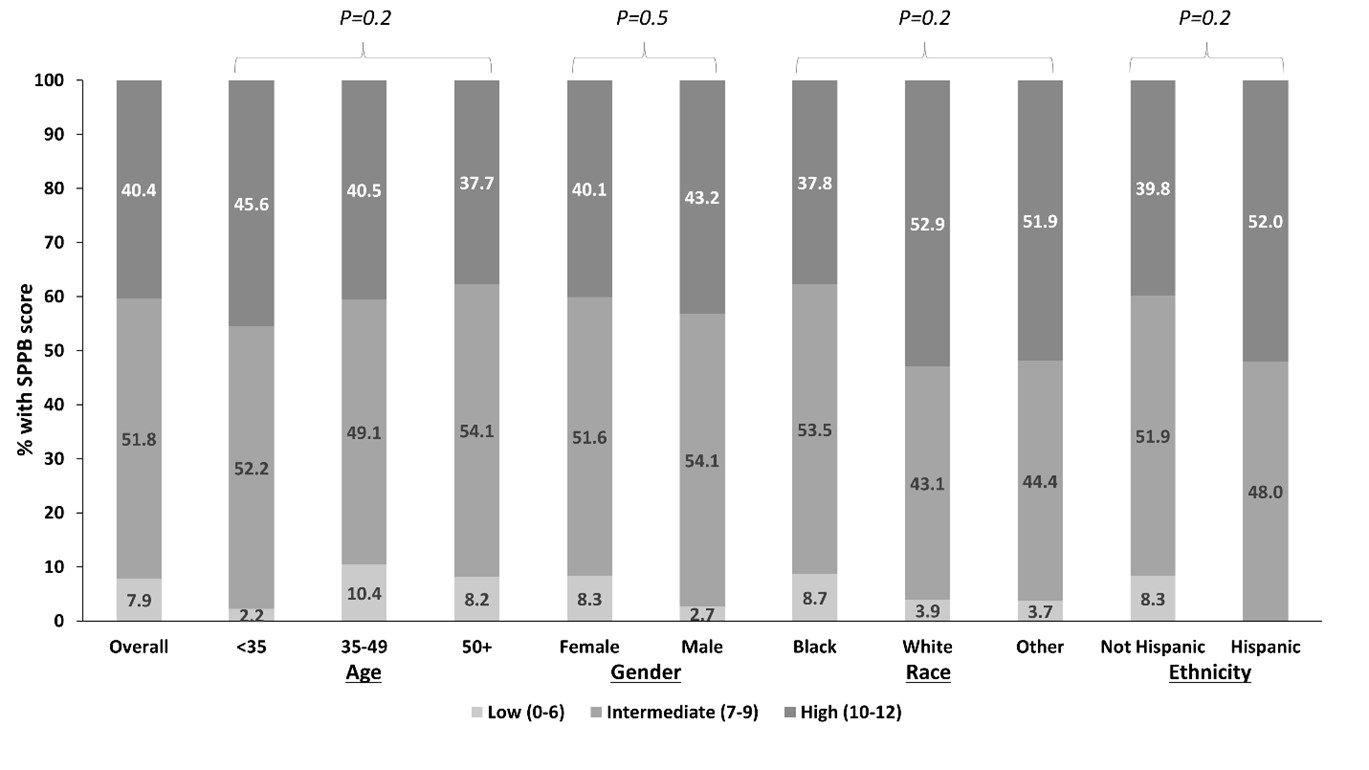
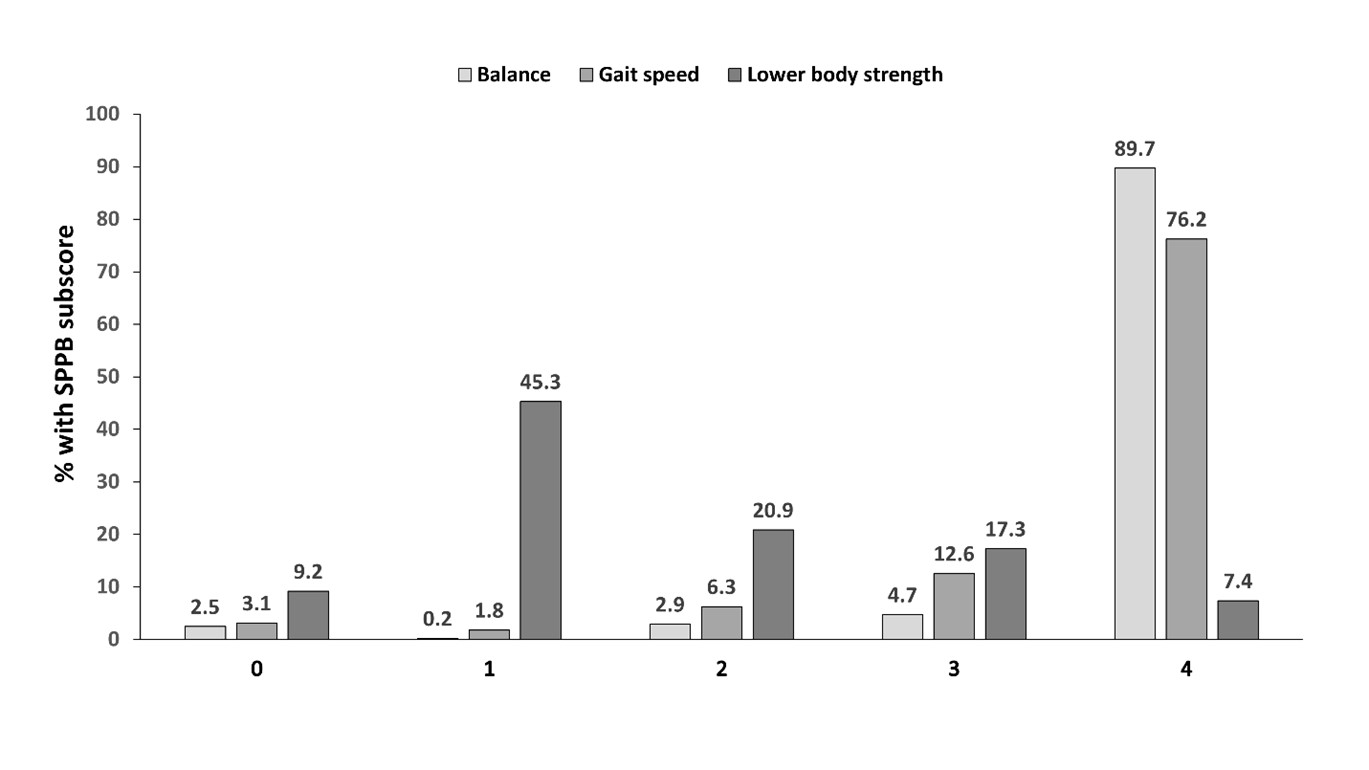
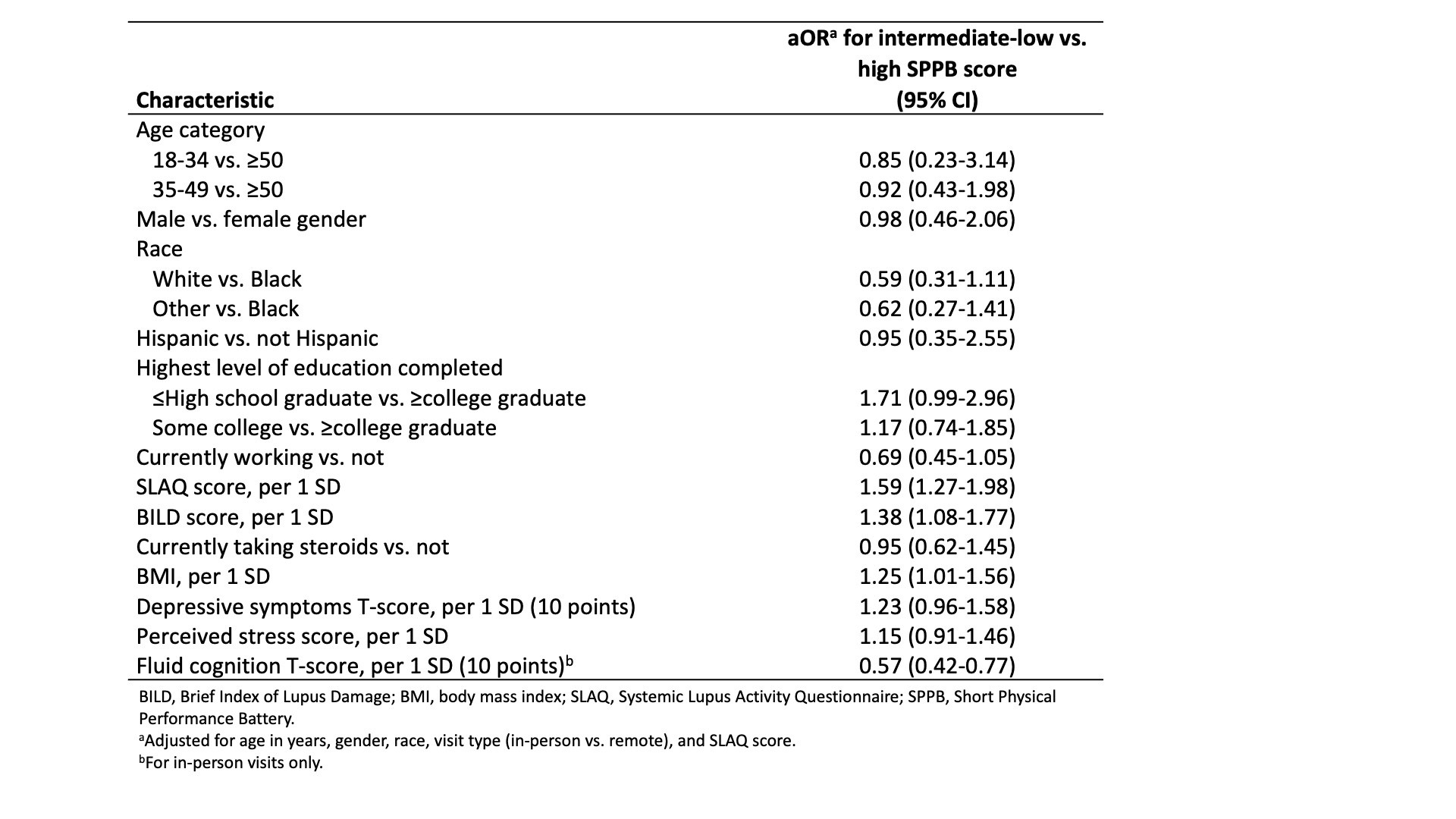
Results: Among 446 participants (mean age 46.2, 91.7% female, and 82.5% Black), more than half (59.6%) had poor (intermediate-low) overall physical performance (Figure 1). Only 7% of the cohort received the maximum score on the lower body strength task, as opposed to 90% and 76% receiving the maximum scores on balance and gait speed tasks, respectively (Figure 2). Current employment status and higher cognitive functioning were associated with 31% and 43% lower odds of intermediate-low physical performance (Table 1). Higher body mass index, disease activity, and disease burden were associated with 25%, 59%, and 38% higher odds of poorer performance, as were higher depressive symptom and perceived stress scores and lower educational attainment.
Conclusion: In our diverse cohort of individuals with SLE, we found a high burden of low to intermediate physical performance and identified SLE- and non-SLE-related factors associated with poorer performance. Clinicians may use these results to identify patients who are most at risk for suboptimal physical performance and intervene to maintain or improve performance levels, which could delay or prevent associated poor outcomes and help ensure continued independence.
Figure 1. Short Physical Performance Battery scores (range 0-12, higher scores indicating higher levels of physical performance) among study participants, overall and by participant demographics.
Figure 2. Short Physical Performance Battery subscores (range 0-4, 0=inability to perform task, 4=highest level of performance) for balance, gait speed, and lower body strength (chair stands) among study participants.
Table 1. Associations of intermediate or low (<10) vs. high (10-12) physical performance scores with participant characteristics.
C. Hoge: None; C. Bowling: None; C. Dunlop-Thomas: None; B. Pearce: None; S. Lim: None; C. Drenkard: None; L. Plantinga: None.