University Medical Center of El Paso El Paso, TX, United States
Disclosure information not submitted.
Yvette Farran1, Mark Hwang1, John Reveille2, Lianne Gensler3, Accelerating Medicines Partnership Program RA SLE Network4, Mariko Ishimori4 and Michael Ward5, 1The University of Texas Health Science Center at Houston McGovern Medical School, Houston, TX, 2The University of Texas Health Science Center, Houston, TX, 3University of California San Francisco, Department of Medicine, Division of Rheumatology, San Francisco, CA, 4Cedars-Sinai Medical Center, Los Angeles, CA, 5National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health, US Department of Health and Human Services, Bethesda, MD
Background/Purpose: Ankylosing Spondylitis (AS) is a chronic inflammatory disease that primarily affects the spine and sacroiliac joints. Depression is a common comorbidity in AS patients and can have a significant impact on their quality of life. The Center for Epidemiologic Studies Depression Scale (CES-D) is a widely used self-report questionnaire for measuring depression in various populations. However, the validity of CES-D in AS patients is unclear.
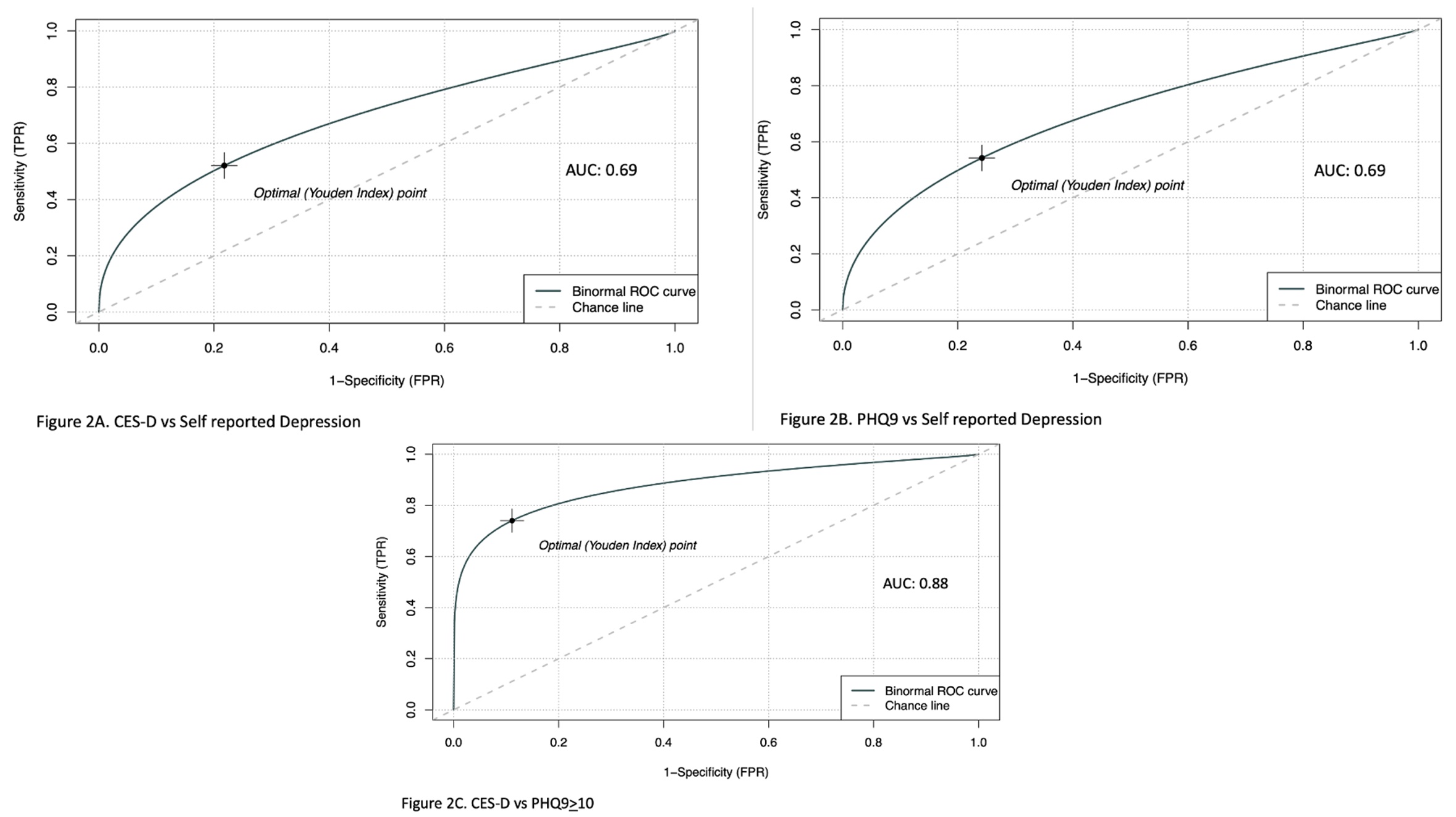
Methods: We investigated the psychometrics of the CES-D in AS by studying Prospective Study of Ankylosing Spondylitis (PSOAS) observational cohort patients with baseline, concomitant PHQ9 and self-reported depression. Construct validity was examined through convergent and known-groups validity. CES-D and PHQ9 was assessed using Pearson’s correlation coefficient. Known groups validity for the CESD was tested using student’s t-test comparing patients with and without self-reported depression. To find the optimal cutoffs, ROC curves were made plotting CES-D against Patient reported depression, PHQ9 against Patient report depression and CES-D against PHQ9≥10. The optimal cutoff point was found using Youden’s index.
Results: 846 of the patients from the PSOAS cohort had completed CES-D at their initial visit. Of those, 325 had completed CES-D, PHQ-9, and self-reported depression. 25% (83/325) had PHQ9 > 10, 34% (112/325) had CES-D > 16 and 17% (56/325) had self-reported depression. Of the patients with self-reported depression, the average CES-D score was 19.8 and the average PHQ9 score was 10.7.The CES-D showed strong correlation with PH9 in AS patients (r > 0.82, p < 0.01) (Figure 1).T-test was significant comparing CES-D scores of AS patients with and without self-reported depression (p< .01) with a mean difference of 7.5 (4.6-10.3 95% CI).The ROC curves are shown in Figure 2. AUC’s of these ranged from: 0.69-0.88. The optimal cut off point for CES-D in these patients based on Youden’s index was 17-18.
Conclusion: In our AS patients, the CES-D scores are valid and have good construct validity. CES-D correlated well with self-reported depression and PHQ9. This suggests that CES-D is valid in this patient population and that a CES-D cutoff of 18, like that found in Rheumatoid Arthritis patients1, may be a better cutoff value to indicate depression in AS patients.
Y. Farran: None; M. Hwang: None; J. Reveille: None; L. Gensler: AbbVie, 2, Acelyrin, 2, Eli Lilly, 2, Fresenius Kabi, 2, Janssen, 2, Novartis, 2, 5, Pfizer, 2, UCB Pharma, 2, 5; A. RA SLE Network: None; M. Ishimori: None; M. Ward: None.



 photo")
.jpg)