Session: (0543–0581) SLE – Diagnosis, Manifestations, & Outcomes Poster I
0543: Sensitivity of the 2019 European Alliance of Associations for Rheumatology /American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus in a Population-based Cohort; A Study Set in Norway 2000-2015
Hilde Haukeland1, Sigrid Reppe Moe1, Cathrine Brunborg2, Antonela Botea3, Nenad Damjanic4, Gro Wivestad5, Heidi Øvreås6, Thea Bøe7, Torhild Garen1, Anniken Orre8, Helga Sanner9, Øyvind Molberg10 and Karoline Lerang9, 1Oslo University Hospital, Department of Rheumatology, Oslo, Norway, 2Oslo Centre for Biostatistics and Epidemiology, Research Support Services, Oslo University Hospital - Rikshospitalet, Oslo, Norway, 3Betanien Hospital, Department of Rheumatology, Skien, Norway, 4Ostfold Hospital Trust, Department of Rheumatology,, Grålum, Norway, 5Hospital of Southern Norway Trust, Division of Rheumatology, Department of Medicine, Kristiansand, Norway, 6Lillehammer Hospital for Rheumatic Diseases, Department of Rheumatology, Lillehammer, Norway, 7Vestfold Hospital Trust, Department of Internal Medicine, Tønsberg, Norway, 8Vestre Viken Hospital Trust, Department of Rheumatology, Drammen, Norway, 9Oslo University Hospital, Department of Rheumatology, Nydalen, Norway, 10University of Oslo, Institute of Clinical Medicine, Oslo, Norway
Background/Purpose: To diagnose Systemic Lupus Erythematosus (SLE), one must understand the phenotype specter and interpret clinical, serological, radiological, and histopathological data, as well as exclude mimicking conditions. As diagnostic criteria for SLE currently are not within reach, patients are selected for research by classification criteria created to define homogeneous SLE-cohorts comparable across studies. This requires high specificity, which typically compromise the sensitivity. The new 2019 European Alliance of Associations for Rheumatology /American College of Rheumatology (ACR) classification criteria for SLE (2019 EA criteria) appears to be significantly more sensitive than the 1997 ACR criteria when applied on cohorts from referral centers/registries, especially for recent onset SLE. However, further studies are needed to confirm this highly promising sensitivity-improvement, not least in population-based SLE cohorts. We established a population-based cohort including all new-onset SLE cases during 1999-2017 in an area of 2.9 million inhabitants in Norway. Then we estimated the sensitivity of 1997 ACR- and 2019 EA criteria for adult cases diagnosed during 2000-2015.
Methods: The cohort included all cases (all ages) ICD-10 coded as SLE in the study area during 1999-2017. All cases were chart-reviewed to confirm/reject SLE diagnosis and assess classification-criteria items at time of diagnosis, and prospectively. At study end, 84% vs. 94% of cases in the total incident cohort fulfilled 1997 ACR- vs. 2019 EA criteria. Applying SLE diagnosis as "gold standard", sensitivity of 1997 ACR- vs. 2019 EA criteria was compared at diagnosis, at two years disease duration, and at study end, in adult incident SLE cases diagnosed during 2000-2015. All tests were two-sided and a 5% significance level was used. We applied 2015 as study end to have complete two-year data, and 2000 as study start as 29 cases diagnosed in 1999 lacked complete follow-up data due to technical reasons.
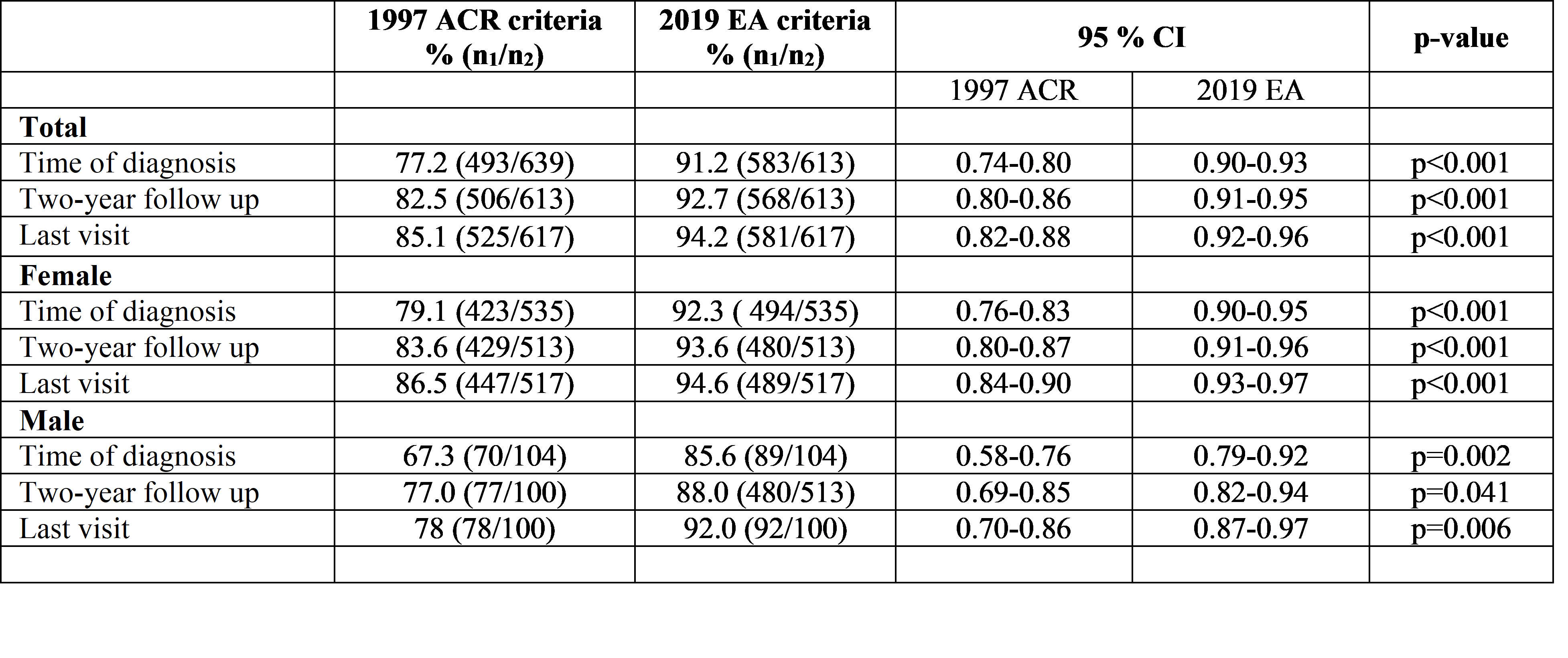
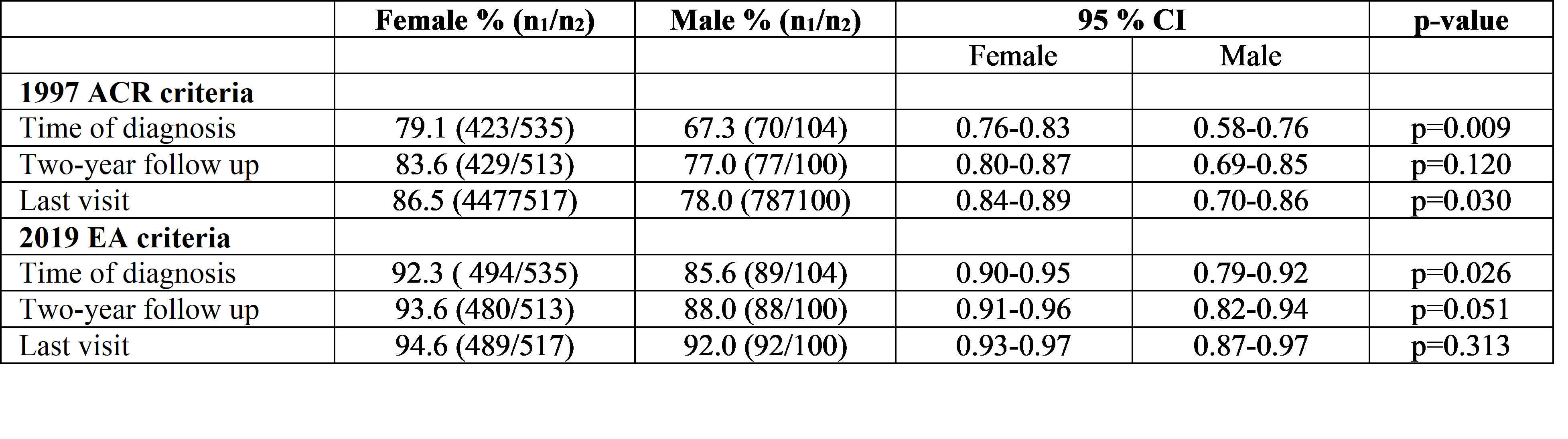
Results: After chart-review the population-based adult SLE cohort included 647 cases with new-onset disease diagnosed during 2000-2015. In this cohort the 2019 EA criteria showed higher sensitivity than the 1997 ACR criteria at diagnosis (91.2% vs. 77.2 %), also when stratified for sex (Table 1A). The sensitivity of the 2019 EA criteria was also superior to the 1997 ACR criteria after two years disease duration and at end of study, for both female-and male subjects (Table 1A). The sensitivity of the 2019 EA criteria was not significantly different for the female vs. the male population (Table 1B).
Conclusion: We provide new evidence for excellent sensitivity of the 2019 EA criteria for new-onset SLE, from a presumably complete population-based cohort. More than 90% of the SLE-cohort cases met the 2019 EA criteria already at time of diagnosis. Stratified for sex, almost all female subjects meeting the 2019 EA criteria during study period did so at time of diagnosis (91.2 % out of 94.2%). The corresponding numbers for the male population was 85% out of 92%.One possible implication for future clinical studies might be capture of almost all SLE patients early in their disease course, which may have important implications for studies on treatment.
Table 1A Comparative sensitivity of classification criteria in the adult incident SLE study population (2000-2015, N=647) N, number of cases in the study population; n1, number of cases fulfilling the criteria; n2, total number of cases at visit
Table 1B Comparative sensitivity of sex in the adult incident SLE study population (2000-2015, N=647) N, number of cases in the study population; n1, number of cases fulfilling the criteria; n2, total number of cases at visit
H. Haukeland: UCB, 1; S. Reppe Moe: None; C. Brunborg: None; A. Botea: None; N. Damjanic: None; G. Wivestad: None; H. Øvreås: None; T. Bøe: None; T. Garen: None; A. Orre: None; H. Sanner: None; Ø. Molberg: None; K. Lerang: None.