Session: Abstracts: Systemic Sclerosis & Related Disorders II: Clinical Research (1699–1704)
1704: Esophageal Mucosal Erosions Can Predict the Deterioration of Lung Function over a Four-year Follow-up Period and Long-term Mortality in Patients with Interstitial Lung Disease Associated with Scleroderma
Catholic University of the Sacred Heart Roma, Rome, Italy
Disclosure information not submitted.
gerlando Natalello1, enrico De Lorenzis1, Ludovica Berardini2, lucrezia verardi1, pier giacomo Cerasuolo1, Alfredo Papa3, Italo De Vitis3, Francesco Varone2, Luca Richeldi2, Maria Antonietta D'Agostino1 and Silvia Bosello1, 1Division of Rheumatology - Catholic University of the Sacred Heart, Fondazione Policlinico Universitario Agostino Gemelli, Rome, Italy, 2Division of Pulmonology - Catholic University of the Sacred Heart, Fondazione Policlinico Universitario Agostino Gemelli, Rome, Italy, 3Division of Gastroenterology - Catholic University of the Sacred Heart, Fondazione Policlinico Universitario Agostino Gemelli, Rome, Italy
Background/Purpose: Interstitial lung disease (ILD) is a major cause of morbidity and disease-related death in systemic sclerosis (SSc). Esophageal disease is common in SSc, and micro-aspiration of gastroesophageal reflux may contribute to the pathogenesis of ILD. The aim of this study is to explore the association of erosive esophagitis (EE) determined by esophagogastroduodenoscopy (EGD) with lung function deterioration and survival in patients with SSc.
Methods: Consecutive patients presenting with symptoms of gastro-esophageal involvement who underwent EGD from 2005 to 2015 were characterized based on the occurrence of EE, following the Los Angeles criteria1, and longitudinally evaluated. Patients with SSc-ILD were assessed over a 48-month period for pulmonary function test deterioration according to OMERACT criteria2. Both raw and SSc-associated mortality were documented over a ten-year period for the entire cohort. SSc patients, with or without EE, were compared though survival analysis. A competing risk survival analysis was specifically performed to investigate the association of EE with SSc-related mortality with death due to alternative causes as competing event.
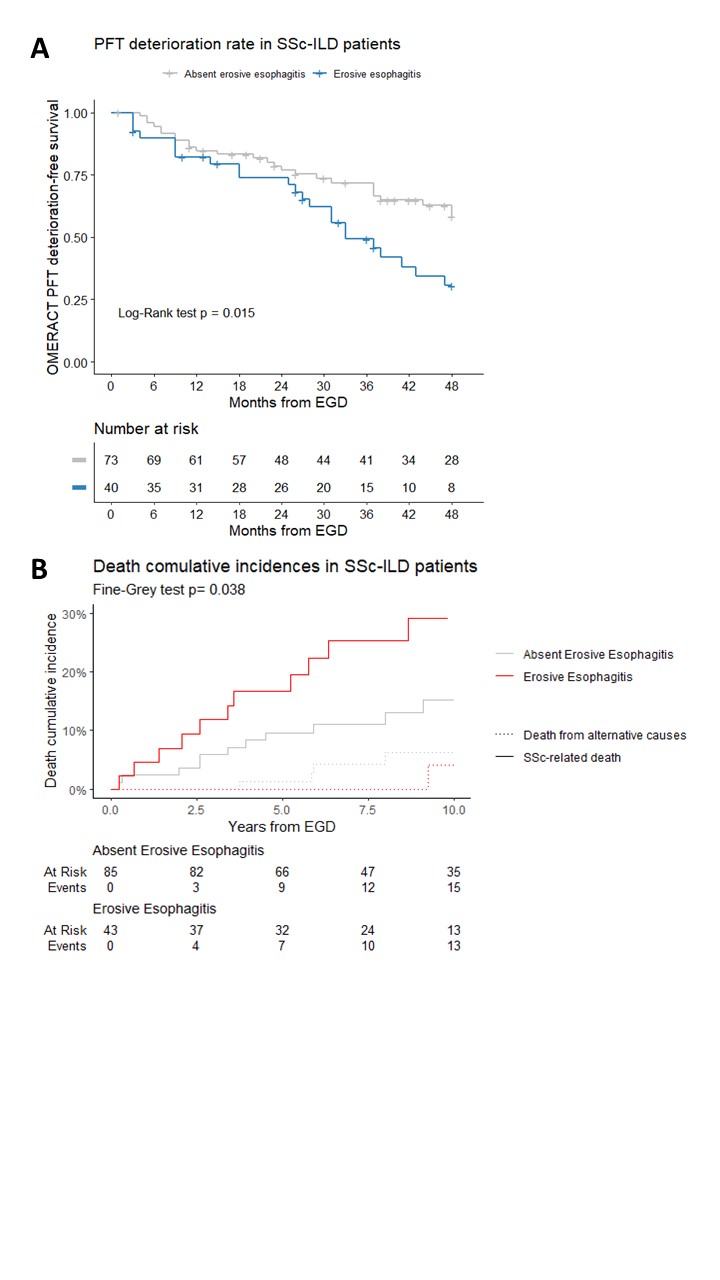
Results: Of the 214 SSc patients studied, 9.8% were male, the mean age was 58.8±13.5 years, the median disease duration was 5.0 years (IQR 1.0-9.0), and the diffuse variant was present in 36.9%. Out of these patients, 33.6% had EE and 59.8% had ILD and no association was found between these two disease characteristics. Forty-nine SSc-ILD patients experienced OMERACT deterioration. EE was associated with a reduced OMERACT progression-free survival (Log-Rank p=0.015) (Fig.A) and an independently doubled risk of progression (HR 1.97, 95% CI 1.09-3.55 adjusted for age, gender, digital ulcers, disease duration, p=0.025). In the overall cohort, fifty-one deaths were reported, 37 of which were SSc-related. In the ILD group, there were a total of 27 deaths due to any cause, with 23 specifically due to SSc. EE was associated with the risk of SSc-related death in the ILD group (HR 2.08, 95% CI 1.05-5.28, Fine-Gray p=0.038) (Fig.B), but not in SSc patients without ILD.
Conclusion: In our cohort, EE represents a risk factor for functional deterioration and SSc-related long-term mortality specifically in SSc patients with ILD, supporting a detrimental role of gastro-esophageal micro-aspiration in exacerbating lung fibrosis.
g. Natalello: None; e. De Lorenzis: None; L. Berardini: None; l. verardi: None; p. Cerasuolo: None; A. Papa: None; I. De Vitis: None; F. Varone: None; L. Richeldi: None; M. D'Agostino: AbbVie/Abbott, 2, 5, 6, Amgen, 2, 5, 6, Bristol-Myers Squibb(BMS), 2, 5, 6, Celgene, 2, 5, 6, Eli Lilly, 2, 5, 6, Janssen, 2, 5, 6, Merck/MSD, 2, 5, 6, Novartis, 2, 5, 6, Pfizer, 2, 5, 6, UCB, 2, 5, 6; S. Bosello: None.