Helena Achten1, Liselotte Deroo2, Kristel De Boeck3, Matthias Jarlborg1, Tine Decruy1, Joke Deprez1, Emilie Dumas1, Dirk Elewaut4 and isabelle peene5, 1Ghent University, Ghent, Belgium, 2Ghent University, Gent, Belgium, 3Ghent University Hospital, Ghent, Belgium, 4Ghent University and VIB Center for Inflammation Research, Ghent, Belgium, 5University Hospital Ghent, Ghent, Belgium
Background/Purpose: Loss of galactose and sialic acid structures attached to the IgG-Fc-fragment switches the antibody effector function from anti-inflammatory to pro-inflammatory1. This study investigated the IgG- Fc-N-glycosylation profiles in patients from the Belgian Sjögren's Syndrome Transition Trial (BeSSTT) in relation to disease state, salivary gland ultrasonography SGUS) and histopathology, and autoantibodies against SSA (Ro52/Ro60) and SSB.
Methods: The relative amount of N-sialylated and N-galactosylated IgG was determined by capillary electrophoresis after using the endo-S glycosidase based assay. 300 serum samples of patients of the BeSSTT, an observational cohort of patients with definite pSS (n=177), fulfilling the 2016 ACR/EULAR classification criteria, and of patients with suspected pSS (n=111) due to presence of either objective sicca or one immunological criterion, were investigated. Groups were made based on the presence or absence of sicca complaints, objective sicca, anti-SSA reactivity and histopathology focus score. SGUS was assessed by Hocevar Score, categorized in negative (0-14), low positive (15-26) and high positive (27-48)2. Differences in levels of IgG-Fc-N-sialylation and -galactosylation were determined using Kruskal-Wallis testing. P-values ≤0.05 were considered statistically significant. Bonferroni correction was applied for post-hoc analyses.
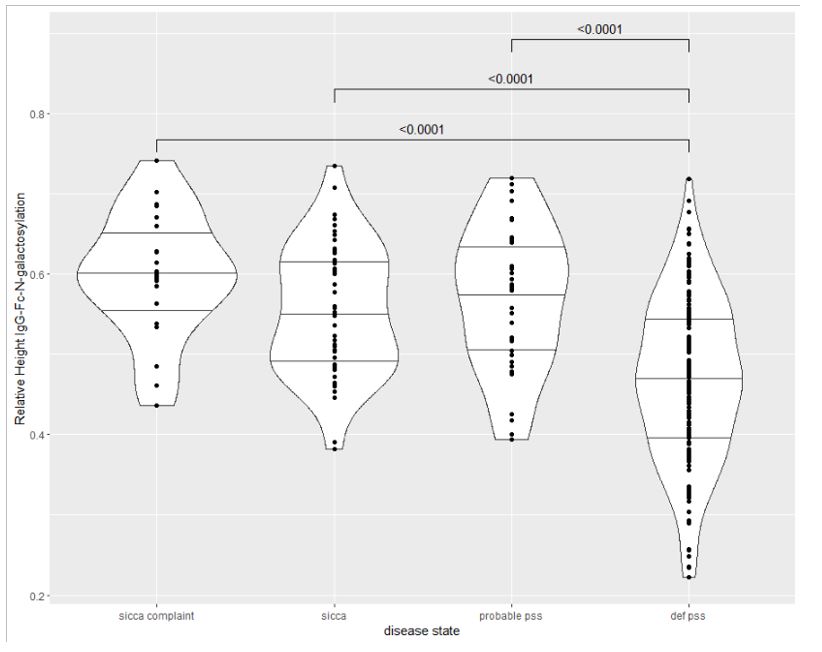
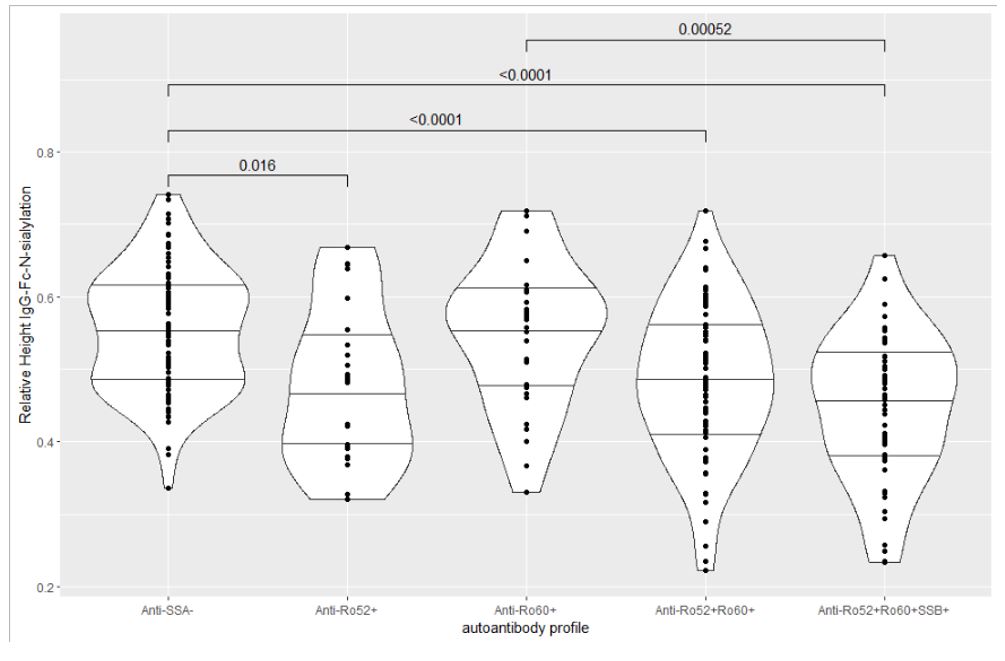
Results: IgG-Fc-N-sialylation and -galactosylation were significantly lower in definite pSS than in patients with sicca complaints, objective sicca or anti-SSA/SSB reactivity only (probable pSS) (Fig 1). Besides, IgG-Fc-N-sialylation and IgG-Fc-N-galactosylation were significantly lower in high positive SGUS- versus low positive and negative SGUS-scores and in positive versus negative focus scores. IgG-Fc-N-sialylation and -galactosylation were significantly lower in anti-Ro52+Ro60+SSB+, anti-Ro52+Ro60+ and anti-Ro52+ patients than in anti-SSA-/SSB- patients. Strikingly, IgG-Fc-N-sialylation and -galactosylation were also significantly higher in anti-Ro52+60+ and anti-Ro52+Ro60+SSB+patients than in anti-Ro60+ patients (Fig 2). Results are shown in Table 1.
Conclusion: There was a gradual loss of IgG-Fc-N-sialic acid and IgG-Fc-N-galactose as the disease became more prominent, as observed from sicca and probable pSS to definite pSS. The IgG-Fc-N-glycosylation profile was associated with the degree of salivary gland damage in pSS. Anti-Ro52+Ro60+SSB+, Anti-Ro52+Ro60+ and Anti-Ro52+ patients had a more pro-inflammatory IgG-Fc-N-glycosylation profile than anti-SSA- and strikingly also than anti-Ro60+ patients.
Table 1. Relative amount of Fc-N-sialylated and Fc-N-galactosylated IgG in relation to disease state, salivary gland damage (SGUS and histopathology) and autoantibody profile.
Figure 1. IgG- Fc-N-galactosylation in function of disease state
Figure 2. IgG-Fc-N-galactosylation level in function of autoantibody profile
H. Achten: None; L. Deroo: None; K. De Boeck: None; M. Jarlborg: None; T. Decruy: None; J. Deprez: None; E. Dumas: None; D. Elewaut: AbbVie/Abbott, 6, Bristol-Myers Squibb(BMS), 5, Eli Lilly, 2, galapagos, 5, Janssen, 6; i. peene: argenx, 1, Eli Lilly, 6, Janssen, 6.



.jpg)