Chris Lane1, Lauren Mihalek2, Kelli Allen3, Beth Jonas4, Patti Katz5 and Louise Thoma6, 1UNC Chapel Hill, Chapel Hill, NC, 2University of North Carolina - Chapel Hill, Chapel Hill, NC, 3University of North Carolina, Durham, NC, 4University of North Carolina at Chapel Hill, Chapel Hill, NC, 5University of California San Francisco, San Rafael, CA, 6University of North Carolina, Chapel Hill, NC
Background/Purpose: Adults with rheumatoid arthritis (RA) often experience functional limitations (e.g., difficulty walking, dressing oneself), even with low disease activity and good pharmaceutical management. Rehabilitation services (i.e. physical therapy and occupational therapy) improve function, yet rehabilitation service use is low among adults with RA. Taken together, this suggests that many adults with RA are underserved by rehabilitation, conservatively defined as high functional burden (moderate-severe functional limitation) with no prior use of rehabilitation for RA. To better understand the gaps in care, we must understand rehabilitation use among those with functional needs and identify characteristics associated with being underserved. The purpose of this study was to examine the associations of demographic and clinical characteristics with being underserved by rehabilitation among adults with RA.
Methods: Data were cross-sectionally collected from online surveys from patients with RA who received care at UNC Health rheumatology clinics in 2020 and 2021. The primary outcome was being underserved by rehabilitation, which was defined as reporting moderate-severe functional limitation (PROMIS PF10a score < 40) and never previously using rehabilitation services related to RA (self-reported use yes vs. no). The demographics and clinical exposure variables were race and ethnicity (non-Hispanic Black, non-Hispanic White, Hispanic of any race), gender (women, men), health insurance (private, Medicare, Medicaid, none), income (higher [exceeding basic needs], lower [not exceeding basic needs]), education status (higher [at least some college], lower [no college]), work status (disabled, other), and BMI (normal, overweight, obese). We calculated the proportion of the sample with moderate-severe functional limitation, no prior rehabilitation use for RA, and underserved by rehabilitation. We examined associations of the exposure variables with being underserved using logistic regression models adjusted for self-reported age, disease duration, and joint replacement. Odds ratios and 95% confidence intervals were presented.
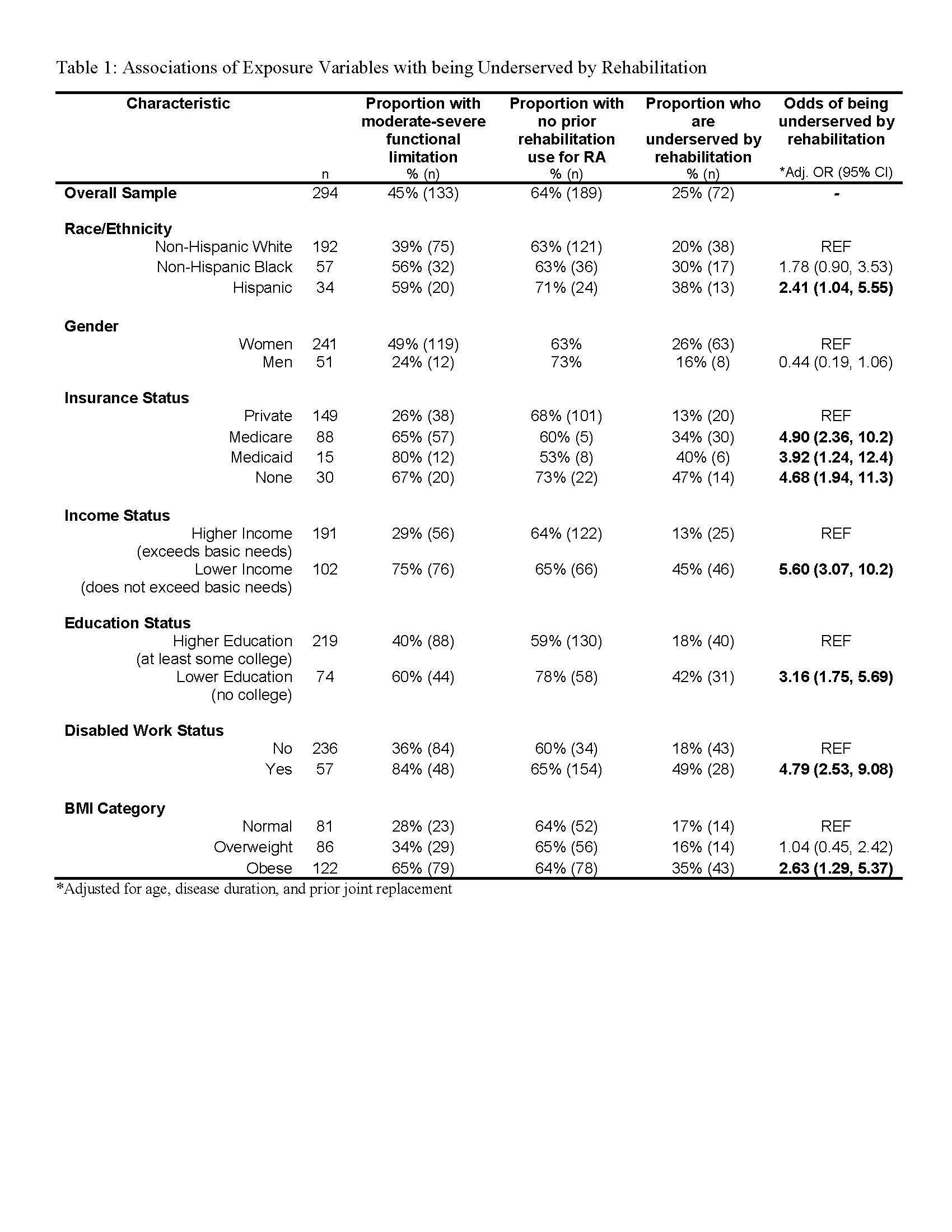
Results: Of 294 adults with RA who participated (age 56.3±14.2 years, disease duration 10.1±10.7 years), 45% reported moderate-severe functional limitation, 64% never used rehabilitation services related to RA, and 25% were underserved by rehabilitation. The following characteristics were strongly associated (adjusted OR range 2.4-5.6) with being underserved by rehabilitation: Hispanic ethnicity (compared to Non-Hispanic White), Medicare, Medicaid, or no health insurance (compared to private insurance), lower income (compared to higher), lower education (compared to higher), disabled work status (compared to other work status), and obesity (compared to normal weight), as detailed in Table 1.
Conclusion: Strikingly, at least one in four adults with RA were underserved by rehabilitation using a conservative definition. There is a clear unmet need for rehabilitation, particularly in historically marginalized groups. Future work must develop strategies for facilitating rehabilitation referral and use for those with functional needs.
C. Lane: None; L. Mihalek: None; K. Allen: None; B. Jonas: None; P. Katz: None; L. Thoma: None.