Peter Mandl1, Maria-Antonietta D'Agostino2, Victoria Navarro-Compán3, Irina Gessl1, Garifallia Sakellariou4, Abhishek Abhishek5, Fabio Becce6, Nicola Dalbeth7, Hang-Korng Ea8, Emilio Filippucci9, Hilde Berner Hammer10, Annamaria Iagnocco11, Annette De Thurah12, Esperanza Naredo13, Sebastien Ottaviani14, Tristan Pascart15, Fernando Perez-Ruiz16, Irene Pitsillidou17, Fabian Proft18, Juergen Rech19, Wolfgang Schmidt20, Luca Sconfienza21, Lene Terslev22, Brigitte Wildner23, Pascal Zufferey24 and Georgios Filippou25, 1Department of Rheumatology, Medical University of Vienna, Vienna, Austria, 2Universita Cattolica del Sacro Cuore Rome, Courbevoie, France, 3Department of Rheumatology, La Paz University Hospital, IdiPaz, Madrid, Spain, 4Department of Internal Medicine and Therapeutics, Università di Pavia, Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy, 5University of Nottingham, Nottingham, United Kingdom, 6Lausanne University Hospital (CHUV), Lausanne, Switzerland, 7University of Auckland, Auckland, New Zealand, 8Hôpital Lariboisière, APHP-Nord, Service de Rhumatologie, Université de Paris Cité, Paris, France, 9Polytechnic University of Marche, Jesi, Italy, 10Center for Treatment of Rheumatic and Musculoskeletal Diseases (REMEDY), Diakonhjemmet Hospital, Oslo, Norway AND University of Oslo, Faculty of Medicine, Oslo, Norway, 11University of Turin, Roma, Italy, 12Aarhus University Hospital, Aarhus, Denmark, 13Hospital Fundación, Madrid, Spain, 14Assistance Publique Hopitaux de Paris, Paris, France, 15Department of Rheumatology, Saint-Philibert Hospital, Lille Catholic University, Lille, France, 16Rheumatology Division, Osakidetza, OSI-EE Cruces, Cruces University Hospital, Barakaldo, Spain, 17EULAR Patient Research Partner, Executive Secretary of Cyprus League Against Rheumatism, Nicosia, Cyprus, 18Department of Gastroenterology, Infectiology and Rheumatology (including Nutrition Medicine), Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany, 19University Clinic Erlangen, Erlangen, Germany, 20Rheumatology, Immanuel Krankenhaus Berlin, Medical Centre for Rheumatology Berlin-Buch, Berlin, Germany, 21Dipartimento di Scienze Biomediche per la Salute, Università degli Studi di Milano AND IRCCS Istituto Ortopedico Galeazzi, 20161, Milan, Italy, 22Center for Rheumatology and Spine Diseases, Rigshospitalet, Glostrup, Denmark, 23University Library, Medical University of Vienna, Vienna, Austria, 24Rheumatology Department, University of Lausanne, CHUV, Lausenne, Switzerland, 25IRCCS Galeazzi - Sant'Ambrogio Hospital, Milan, Italy
Background/Purpose: The multifaceted clinical presentation in crystal-induced arthropathies (CiA) poses challenges to imaging. Our goal was to formulate evidence-based recommendations on the use of imaging in the diagnosis and management of CiA.
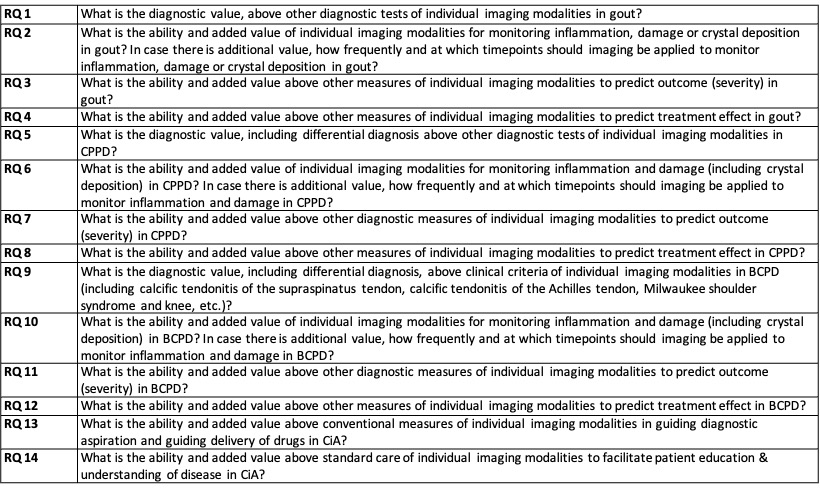
Methods: An international task force of 25 rheumatologists, radiologists, methodologists, health care professionals and patient research partners from 11 countries was formed according to the EULAR standard operating procedures. Fourteen key questions on the role of imaging in the most common forms of CiA were generated (Table 1). The CiA assessed included gout, calcium pyrophosphate dihydrate deposition and basic calcium phosphate deposition. Imaging modalities included conventional radiography, ultrasound, magnetic resonance imaging and computed tomography. Experts applied research evidence obtained from 4 systematic literature reviews using MEDLINE, EMBASE and CENTRAL after assessing for risk of bias. Task force members provided level of agreement (LoA) anonymously by using a numeric scale.
Results: Five overarching principles and 10 recommendations were produced on the role of imaging in making a diagnosis, monitoring inflammation, structural damage and crystal deposition, predicting severity and treatment effect, guiding intervention, and patient education in CiA (Table 2). Level of evidence and grade of recommendation was evaluated. Overall, the LoA for the recommendations was very high (8.5-9.9).
Conclusion: These are the first recommendations that encompass all common forms of CiA and guide the use of established imaging modalities in this disease group.
Table 1. Research questions. BCPD: basic calcium-phosphate deposition; CiA: crystal-induced arthropathy; CPPD: calcium-pyrophosphate deposition; RQ: research question
Table 2. EULAR Recommendations for the use of imaging in crystal-induced arthropathies in clinical practice. *1a for gout, 1a for CPPD, 5 for BCPD; $1a for US, 1a for CR, 1b for CT; #A for gout, A for CPPD, C for BCPD; §A for CR, A for US, B for CT Numbers in column ‘LoA’ indicate the mean and SD (in parenthesis) of the LoA (range 0–10 with 0=‘completely disagree’ to 10=‘completely agree’), BCPD: basic calcium phosphate deposition; CPPD: calcium pyrophosphate dihydrate deposition; DECT: dual-energy computed tomography; GoR: grades of recommendation; LoA: level of agreement; LoE: level of evidence; MTP1: first metatarsophalangeal; n.a., not applicable;




.jpg)
