Mayo clinic, Rochester, MN Canton, OH, United States
Disclosure information not submitted.
Chanakya Kodishala1, Tina Gunderson2, Edward Lovering2, Rakesh Kumar2, Cynthia Crowson2, John Davis2 and Elena Myasoedova2, 1Mayo Clinic Rochester Minnesota, Rochester, MN, 2Mayo Clinic, Rochester, MN
Background/Purpose: Patients with rheumatoid arthritis (RA) have increased risk for Alzheimer's disease and related dementias (AD/ADRD). Recent studies have reported an association between RA disease activity and risk of AD/ADRD, suggesting that inflammation can be an important contributor to this association. It is unknown whether having more RA flares or spending more time in RA flare increases the risk of AD/ADRD incidence. We examined the role of RA flare and remission on the risk of AD/ADRD.
Methods: This population-based study was conducted on an inception cohort of patients with RA who were residents of a geographic area and aged ≥50 years when they met 1987 American College of Rheumatology criteria for RA in 1980-2014 with follow up until 12/31/2019. Flare/remission status was obtained via medical record review. A worsening of disease status requiring initiation/escalation of therapy or a documentation such as 'flare up', 'ongoing' and 'active' in the medical records was considered a 'RA flare'. While remission was defined as absence of disease activity based on documentation such as 'remission', 'quiescent', 'no activity', or swollen and tender joints (≤1) along with normal inflammatory markers. Visits not classified as flare or remission were counted as intermediate activity. Flares were considered to start on the first date they were documented and to resolve halfway to the next visit where the status was changed (definition 1). In definition 2, 'acute flares' were defined to last ≤6 weeks and patients were considered to have intermediate activity from the 6 week point until the next clinical visit. Incident dementia was defined by presence of two ICD9/10 codes for AD/ADRD at least 30 days apart. Cox models with time-dependent covariates were used to assess the association of RA flares with AD/ADRD, adjusting for age, sex and year of RA.
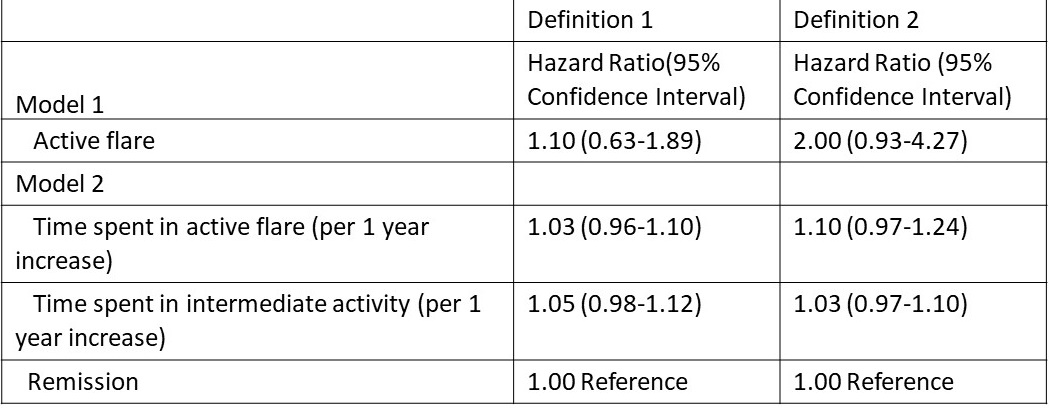
Results: The study included 771 patients with RA (mean age 65.1 years, 65.4% females). During median follow up of 7.7 years, 77 (10%) patients developed AD/ADRD. During a total of 11,085 medical visits (12 median visits per patient), patients were flaring at 3,608 (32.5%) visits and were in remission at 2,631 (23.6%) visits. Median total duration of time spent in RA flare was 46.4 weeks (IQR: 12.9-137.4). Using definition 1, we found no evidence of a higher risk of incident AD/ADRD when in a RA flare vs remission (HR 1.10; 95% CI: 0.63-1.89). Using definition 2, RA flare was associated with a 2-fold higher risk of AD/ADRD (HR 2.00; 95% CI: 0.93-4.27), but this association did not reach statistical significance. When we examined cumulative time spent in each active flare (using either definition of flare) and intermediate activity, we observed a non-significant trend towards increased risk (3-5% per year time spent in active flare or intermediate activity) of incident AD/ADRD compared to time spent in a state of remission (Table).
Conclusion: Our findings indicate that flares of RA disease activity are common and may have a detrimental effect on cognitive status. More studies are needed to understand the mechanisms underlying the association between RA and AD/ADRD, and whether tight control of inflammation and improved flare management in patients with RA may confer long term cognitive benefits.
Table: Association between RA flare and time spent in a flare with incident Alzheimer’s disease and related dementias.
C. Kodishala: None; T. Gunderson: None; E. Lovering: None; R. Kumar: None; C. Crowson: None; J. Davis: Girihlet, 9, Pfizer, 5, Remission Medical, 9; E. Myasoedova: None.