2532: Prevalence and Disease-Specific Factors Associated with Osteoporosis in Systemic Sclerosis: A Cross-Sectional Analysis of Two Large European Cohorts
Charité University Medicine Berlin Berlin, Germany
Disclosure information not submitted.
Charles MIDOL1, Edgar Wiebe2, Elise Siegert3, Dörte Huscher4, Helene Behal5, David Launay6, Eric Hachulla7, Eric Matteson8, Vincent Sobanski9 and Frank Buttgereit2, 1Lille University Hospital, Besançon, France, 2Charité Universitätsmedizin, Dept. Rheumatology, Berlin, Germany, 3Department of Rheumatology, Charité University Hospital, Charité Platz 1, D-10117, Berlin, Germany, 4Institute of Biometry and Clinical Epidemiology and Berlin Institute of Health, Charité Universitätsmedizin Berlin, Berlin, Germany, 5Univ. Lille, CHU Lille, Biostatistics Department, Lille, France, 6Univ. Lille, Inserm, CHU Lille, Service de Médecine Interne, Lille, France, 7CHU Lille, Département de Médecine Interne et Immunologie Clinique, Centre de Référence des Maladies Auto-immunes Systémiques Rares du Nord et Nord-Ouest de France (CeRAINO), Lille, France, 8Mayo Clinic College of Medicine and Science, Rochester, MN, USA, Rochester, MN, 9Univ. Lille, Inserm, CHU Lille, U1286 - INFINITE - Institute for Translational Research in Inflammation, Lille, France
Background/Purpose: Patients with systemic sclerosis (SSc) are at increased risk for osteoporosis (OP) and associated fragility fractures. However, the risks factors and mechanisms driving bone loss in patients with SSc remain elusive. The role of “general” factors such as higher age and low body mass index (BMI) is well established but their interplay with disease-specific factors is unclear. Thus, our objectives in the present study were i) to evaluate the prevalence of clinical OP and fragility fractures in a large population of SSc patients, and ii) to identify potential disease-specific factors for OP in this population. The findings presented in this abstract represent an extended analysis of our previously submitted work, in order to investigate the association between disease severity and osteoporosis in patients with systemic sclerosis.
Methods: This cross-sectional study was based on two large European prospective cohorts of SSc patients with retrospective collection of bone health data. OP was defined as the presence of a T-score below -2.5 at femoral neck or lumbar spine and/or a previous major osteoporotic fracture and/or the prescription of anti-osteoporotic therapy. Long-term therapy with glucocorticoids (GCs) was defined by a daily prednisone equivalent dose above 2.5 mg for more than 3 months. Age, female sex, BMI and treatment with proton pump inhibitors (PPIs) as predefined risk factors according to published evidence, as well as clinically relevant factors associated with a p-value < 0.05 in univariable analyses, after correction for multiple comparison, were implemented into a multivariable logistic regression model.
Results: A total of 932 patients fulfilling the ACR/EULAR 2013 classification criteria were included in the study, followed forward in time at two university hospitals: Lille (n=485) and Berlin (n=447). The two cohorts were studied separately. The prevalence of OP was 32% in Berlin and 23% in Lille (p=0.003), fragility fractures occurred in 22% and 18%, respectively.
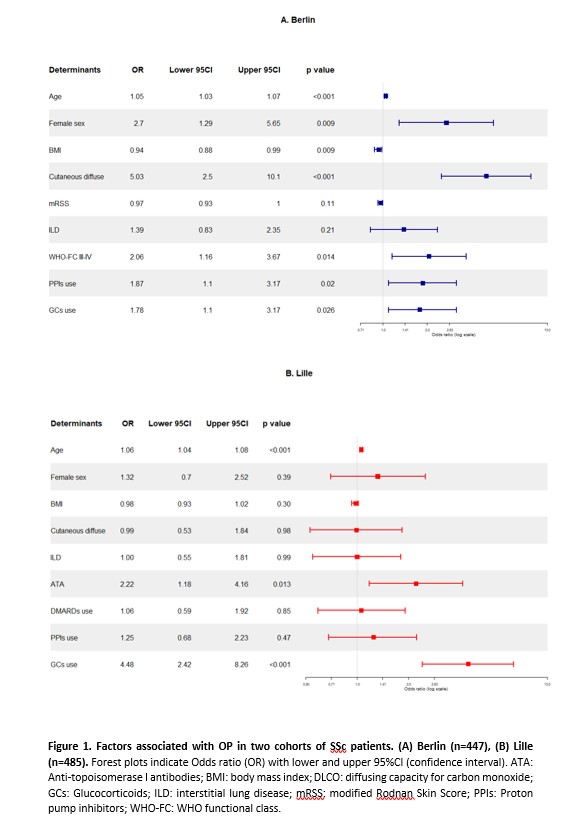
Multivariable analysis in the Berlin cohort indicated that higher age (OR 1.05 [95%CI 1.03 to 1.07], p< 0.001), female sex (OR 2.70 [95%CI 1.29 to 5.65], p=0.009), diffuse skin extent (OR 5.03 [95%CI 2.50 to 10.10], p< 0.001), low BMI (OR 0.94 [95%CI 0.88 to 0.99], p=0.009), WHO-FC III-IV dyspnea (OR 2.06 [95%CI 1.16-3.67], p=0.014), receiving GCs (OR 1.78 [95%CI 1.10 to 3.17], p=0.026) or PPIs (OR 1.87 [95%CI 1.10 to 3.17], p=0.020) were associated with OP.
In the Lille cohort, multivariable analysis confirmed the association of OP with higher age (OR 1.06 [95%CI 1.04 to 1.08], p< 0.001), GCs use (OR 4.48 [95%CI 2.42 to 8.26], p< 0.001), and with anti-topoisomerase I antibody positivity (OR 2.22 [95%CI 1.18 to 4.16], p=0.013).
Conclusion: Our data support a multifactorial etiopathogenesis of OP in SSc: besides common risk-factors for OP such as higher age, female sex, and BMI, several disease specific characteristics were associated with OP, such as SSc severity as reflected by diffuse skin extent and presence of antitopoisomerase I antibodies as well as severe dyspnea and SSc treatment (PPIs and GCs). These findings help to identify patients with SSc at particular risk for OP in clinical practice.
C. MIDOL: None; E. Wiebe: EW reports consultancy fees, honoraria and travel expenses from Medac and Novartis., 2, 6, 12, Travel Expenses; E. Siegert: None; D. Huscher: None; H. Behal: None; D. Launay: Actelion, 5, Boehringer-Ingelheim, 5, CSL Behring and Biocryst, 5, GlaxoSmithKlein(GSK), 5, Takeda, 5; E. Hachulla: Bayer, 6, Boehringer-Ingelheim, 6, CSL Behring, 5, GlaxoSmithKlein(GSK), 5, 6, Johnson & Johnson, 5, 6, Roche, 5, 6, Sanofi-Genzyme, 6; E. Matteson: AbbVie, 5, Alvotech Inc., 2, American College of Rheumatology, 12, Committee member, Boehringer-Ingelheim, 2, 6, Horizon Therapeutics, 1, NIH/NIAMS, 1, Practice Point Communications, 6, UpToDate, 9; V. Sobanski: None; F. Buttgereit: AbbVie/Abbott, 6, Horizon Therapeutics, 5, Pfizer, 5, 6, Roche, 6.