1608: Plasma Proteomic Profiling in Antiphospholipid Antibody-positive Patients with Different Clinical Phenotypes: Results from the Antiphospholipid Syndrome Alliance for Clinical Trials and International Networking (APS ACTION) Registry
Ayesha Butt1, Rolando Garcia Milian1, George Goshua1, Sean Gu1, Eugenia Chock2, Valentina Restrepo1, John Hwa1, Hyung Chun1, H Michael Belmont3, Kello Nina4, D. Ware Branch5, Michelle Petri6, Jason Knight7, Rohan Willis8, Maria Laura Bertolaccini9, Doruk Erkan10, Alfred lee1, Anish Sharda1 and Alexander Pine11, 1Yale School of Medicine, New Haven, CT, 2Yale School of Medicine, Greenwich, CT, 3NYU School of Medicine, New York, NY, 4Northwell Health, Brooklyn, NY, 5University of Utah, Salt Lake City, UT, 6Department of Medicine, Division of Rheumatology, Johns Hopkins University School of Medicine, Timonium, MD, 7University of Michigan, Ann Arbor, MI, 8University of Texas Medical Branch, Galveston, TX, 9King's College London, London, United Kingdom, 10Hospital for Special Surgery, New York, NY, 11VA Connecticut/Yale School of Medicine, West Haven, CT
Background/Purpose: Antiphospholipid syndrome (APS) is an autoimmune disease with thrombotic and obstetric complications arising via a model of immunothrombosis. Patients may present with a spectrum of phenotypes, including thrombotic (tAPS), obstetric (oAPS), or catastrophic/microvascular APS (C/MAPS), while others may have antiphospholipid antibodies (aPL) without disease manifestations. Mechanisms underlying the development of these diverse phenotypes remain uncertain. Proteomic profiling was used in other thrombotic and microvascular disorders to highlight potential mechanisms of disease pathogenesis and may have a role in understanding the pathophysiology of APS.
We performed multiplex plasma proteomic profiling in aPL-positive patients with different clinical phenotypes to gain a greater understanding of potential immunothrombotic mechanisms in the pathogenesis of APS.
Methods: A web-based data capturing system was used to store patient demographics, history, and medications. The inclusion criteria were positive aPL per Updated Sapporo Classification Criteria tested within 1 year prior to enrollment. Multiplex proteomic profiling measuring approximately 7,000 unique proteins (SomaLogic; Boulder, CO, USA) was performed on 40 primary aPL-positive patient plasma samples from APS ACTION Registry (10 each of tAPS with/without oAPS, oAPS only, C/MAPS, and positive aPL without APS classification), and 10 of healthy controls. Differentially abundant proteins among all phenotypic groups and in pairwise comparisons were determined by applying ANOVA and t-tests to log-normalized data, respectively, with p< 0.05 considered statistically significant. Tests were adjusted for false discovery to minimize the likelihood of false positives.
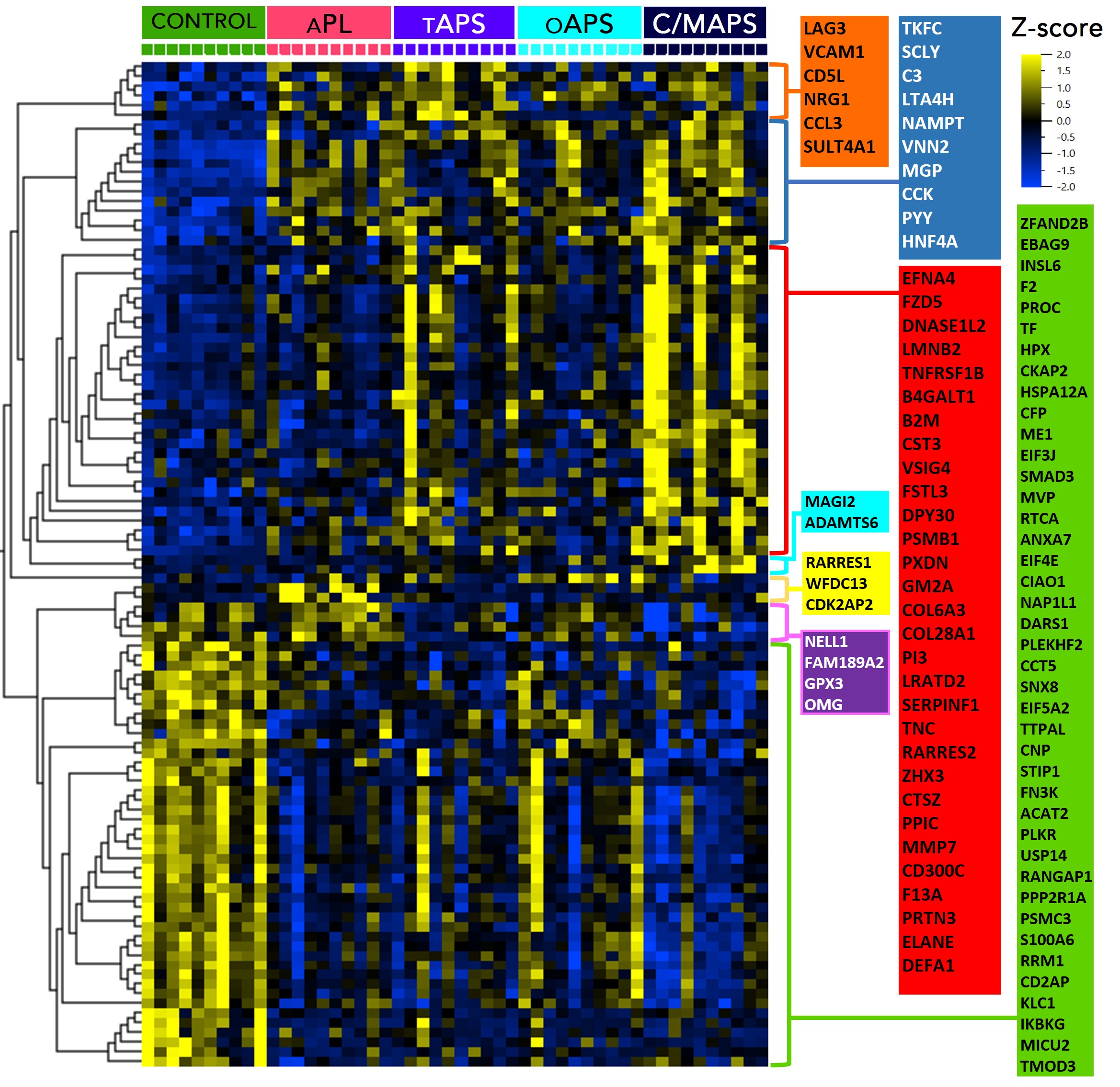
Results: The median age of patients was 48 years; 30% were men, 70% had triple aPL-positivity, and no one had a concurrent diagnosis of lupus. A set of concordant and differentially abundant proteins clustered patients with 4 APS clinical phenotypes and controls (Figure A) with a high statistical significance (p < 0.0007) and a high false discovery confidence (q < 0.05). Pathway enrichment analysis of proteins in the identified set revealed involvement of several pathways such as neutrophil degranulation (p < 10-10), humoral immune response (p < 10-9), coagulation (p < 10-6), alternative complement (p < 10-5) and others (Figure B). Pairwise analyses of APS subtypes revealed increasing abnormalities in these pathways with worsening APS severity, but distinctly in cellular processes such as endocytosis/vesicle-mediated transport, receptor signaling, signal transduction and cellular differentiation (Figure C). This was particularly striking in C/MAPS subtype, with members of negative regulation of inflammatory response and cellular differentiation processes being the only distinction between tAPS and C/MAPS.
Conclusion: Plasma proteome of several APS subtypes is characterized by alteration in peripheral blood cellular processes, particularly receptor signaling, signal transduction and regulation of cellular differentiation, in addition to significant neutrophil, complement, coagulation and cytokine activation notable in all aPL-positive patients.
Figure A. Differentially abundant proteins by APS types and control subjects; APL, non-thrombotic APS (antibodies only); TAPS, thrombotic APS; OAPS, obstetric APS; CAPS/MV, catastrophic /microvascular APS. ANOVA on log-normalized data (p<0.0007, FDR q<0.05). FDR, false discovery rate.
Figure B. Pathways enrichment analysis of proteins from Figure A.
Figure C. Differentially abundant proteins by APS in pairwise comparisons between APS types; APL (non-thrombotic APS, antibodies only), p<0.01; TAPS (thrombotic APS), p<0.01; CAPS/MV (catastrophic /microvascular APS), p<0.005. T-tests on log-normalized data.
A. Butt: None; R. Garcia Milian: None; G. Goshua: None; S. Gu: None; E. Chock: None; V. Restrepo: None; J. Hwa: None; H. Chun: None; H. Belmont: Alexion, 6, Aurinia, 6; K. Nina: None; D. Branch: UCB Pharmaceuticals, 5; M. Petri: Alexion, 1, Amgen, 1, AnaptysBio, 1, Annexon Bio, 1, Argenx, 1, Arhros-Focus Med/Ed, 6, AstraZeneca, 1, 5, Aurinia, 1, 5, 6, Axdev, 1, Biogen, 1, Boxer Capital, 2, Cabaletto Bio, 2, Caribou Biosciences, 2, CVS Health, 1, Eli Lilly, 1, 5, Emergent Biosolutions, 1, Exagen, 5, Exo Therapeutics, 2, Gilead Biosciences, 2, GlaxoSmithKlein(GSK), 1, 5, 6, Horizon Therapeutics, 2, Idorsia Pharmaceuticals, 2, IQVIA, 1, Janssen, 1, 5, Kira Pharmaceuticals, 2, MedShr, 6, Merck/EMD Serono, 1, Momenta Pharmaceuticals, 2, Nexstone Immunology, 2, Nimbus Lakshmi, 2, Proviant, 2, Sanofi, 2, Sinomab Biosciences, 2, Thermofisher, 5, UCB, 2; J. Knight: Jazz Pharmaceuticals, 2; R. Willis: None; M. Bertolaccini: None; D. Erkan: Abbvie, 1, ACR/EULAR, 5, APS ACTION, 12, Executive Committee Co-chair, Argenx, 1, Aurinia, 6, Chugai, 1, Exagen, 5, GSK, 5, 6, NIH-NIAID, 5, Up-To-Date, 9; A. lee: None; A. Sharda: None; A. Pine: None.



.jpg)
.jpg)
